Last updated:
March 9, 2026
Overview
Sarcoidosis is a multi-systemic inflammatory disease characterized by non-caseating granulomas. It is of unknown etiology and predominantly affects the lungs and surrounding lymph nodes. Important differential diagnoses for granulomas need to be made when sarcoidosis is suspected, and these include berylliosis, fungal infections, and malignancy. The presence of involvement of two or more organs is more supportive of its diagnosis.
Epidemiology
- Affects women more than men
- More common in the black population
- Highest age of incidence: 20s – 30s
Clinical manifestations
- Often asymptomatic
- Respiratory symptoms: cough, dyspnea, shortness of breath
- Constitutional symptoms: fever, malaise, lack of appetite, weight loss
- Extrapulmonary symptoms: Dependent on the affected organ systems
- Eyes: uveitis
- Skin:
- Erythema nodosum
- Lupus pernio which is a rash presenting as red indurated plaques with discoloration of the nose, cheeks, and ears
- Nervous system: cranial nerve palsies, diabetes insipidus, meningitis, etc.
- Musculoskeletal: arthralgias and arthritis
- Cardiac: restrictive cardiomyopathy, arrhythmias, pericardial effusion, etc.
- Kidneys: acute interstitial nephritis, nephrolithiasis, nephrocalcinosis
- Liver: hepatic granulomas, hepatomegaly
- Bone marrow and spleen: lymphopenia, anemia, splenomegaly
- Granulomas make the enzyme 1-α-hydroxylase, a rate-limiting enzyme in vitamin D synthesis.
- This leads to increased levels of 1, 25- hydroxyvitamin D which increases intestinal absorption of calcium, leading to hypercalcemia with a suppressed parathyroid hormone.
- Therefore, hypercalcemia is a potential manifestation of sarcoidosis and serum calcium should be evaluated in the lab investigations.
- Granulomas may produce this enzyme thereby increasing its serum levels
- However, it is not clinically significant.
Diagnostics
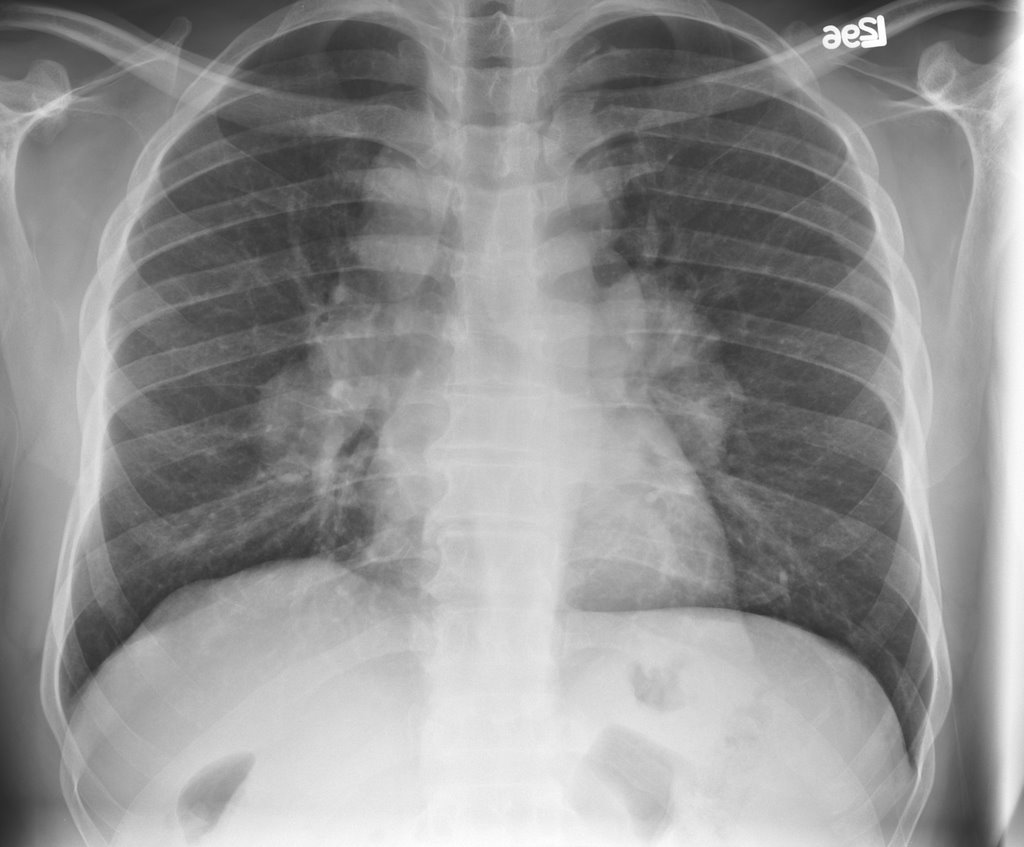
- Best initial test: Chest X-ray
- Findings: bilateral hilar lymphadenopathy with/ without pulmonary infiltrates
- Most accurate test: Biopsy. Can be transbronchial or enlarged lymph node biopsy
- Findings: Non-caseating granulomas
- High-resolution CT: Done for patients with confirmed or suspected sarcoidosis. Findings:
- Bilateral hilar lymphadenopathy
- Peri-bronchial thickening
- Fibrosis
- Other tests:
- CBC: Leukopenia, anemia
- Inflammatory markers (ESR, CRP): elevated
- Serum calcium: elevated
- Serum angiotensin-converting enzyme (ACE): elevated
- Bronchioalveolar lavage (BAL): increased CD4+/ CD8+ ratio (> 3.5). Highly specific.
- Pulmonary function tests (PFTs): restrictive pattern
- To evaluate for multi-organ involvement: LFTs, UECs, urinalysis (Hypercalciuria), ECG (arrhythmias), etc.
- It is also important to rule out the main differentials eg screen for TB
Differential diagnosis
- Berylliosis: usually in an older patient with a known occupational exposure eg. beryllium metal, working in nuclear or aerospace industries
- Tuberculosis: immunocompromised, with previous exposure to TB infected persons
- Hodgkin lymphoma: previous history of infection with mononucleosis
- Non-Hodgkin lymphoma: EBV infection, or history of cell damage (immunosuppressive therapy, radiation)
- Pneumoconiosis: exposure to mineral dust eg. silica
- Histoplasmosis: AIDS patient, exposure to bird or bat excrement, caseating granulomas.
- Granulomatosis with polyangiitis
Treatment
- It is based on the level of symptoms and the extent of organ involvement:
- Most patients with pulmonary sarcoidosis do not require immunosuppressive therapy
- Immunosuppressive therapy is indicated for symptomatic progressive disease, persistent pulmonary infiltration, and progressive decline of lung function
- The first line of treatment is glucocorticoids, eg. prednisone
- If glucocorticoids fail, disease-modifying anti-rheumatic drugs (DMARDs) may be used eg. methotrexate or azathioprine
- Organ transplant may be indicated in severe, chronic, and refractory disease
- Patients should also receive individualized supportive care eg. analgesia, supportive ventilation, supplemental oxygen