Last updated:
March 9, 2026
Overview
Lung cancer refers to tumors from respiratory epithelium, including bronchi, bronchioles, and alveoli. Globally, it is the most commonly diagnosed cancer and the leading cause of cancer deaths among both sexes combined. It occurs more in males than in females, however other subtypes such as adenocarcinoma occur more in women. Lung cancer most commonly presents later on in life, with the highest incidence occurring between the ages of 55-65 years. Patients’ 5-year survival rate is around 15%, and therefore lung cancer often has a poor prognosis.
Etiology
- Tobacco smoking
- Prolonged exposure to cigarette smoke, especially in active smokers is the main risk factor.
- Passive smoking also contributes to the risk.
- It is important to calculate the patient’s cigarette pack-years when evaluating risk:
- Pack-year cigarette history= quantity of cigarettes a person smoked per day/ number of cigarettes in a pack (usually 20) x the number of years of cigarette consumption
- Chronic obstructive pulmonary disease: already a disease commonly caused by chronic tobacco smoking, it increases the risk of lung cancer
- Occupational and environmental exposure: to radon or asbestos
- Exposure to radiation i.e. previous thoracic radiation
Classification
WHO Classification
- WHO classifies lung cancer into two broad categories, which are:
- Non-small cell lung cancer (NSCLC)
- Lung neuroendocrine tumors
Classification according to location of the lesion
- This is divided into two:
- Central with endobronchial growth
- Peripheral with pleural involvement
Histology
- Histologically, we can divide lung cancer into small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC).
- These types majorly determine treatment options as well as having prognostic value.
SCLC
- Has a very strong correlation with smoking
- Has neuroendocrine properties, which means it often leads to the production of specific peptide hormones. These include:
- Adrenocorticotrophic hormone (ACTH)
- Arginine vasopressin (AVP)
- Atrial natriuretic peptide (ANP)
- Gastrin-releasing peptide
- Associated paraneoplastic syndromes include Lambert Eaton myasthenia syndrome and Syndrome of inappropriate antidiuretic hormone secretion
- It is initially very responsive to combined chemotherapy and radiation, however, it commonly relapses.
- Managed primarily by chemotherapy with or without radiation, surgery usually not curative because it is usually spread by the time of diagnosis
- Has a worse prognosis than NSCLC, as it is rapidly metastasizing
NSCLC
- Has the following subtypes:
- Lung adenocarcinoma (oat cell)
- Lung squamous cell carcinoma (epidermoid)
- Large cell carcinoma
- Lung adenocarcinoma:
- Most commonly occurring subtype in non-smokers, including women and young patients
- Often causes a pleural effusion
- Associated with Pancoast tumors which lead to Horner’s syndrome
- Includes bronchioalveolar carcinoma (BAC):
- Growth along the alveoli without invasion
- Presents as either a single mass, diffuse multinodular lesion, fluffy infiltrate
- CT shows mass with ground-glass appearance
- Can be mucinous or non-mucinous
- Lung squamous cell carcinoma:
- Strong association with smoking
- Shows cavitations on imaging
- Strongly associated paraneoplastic syndrome is hypercalcemia
- Due to secretion of a parathyroid hormone-like peptide
- Leads to an increase in serum calcium and a subsequent fall in parathyroid hormone levels
- Large cell carcinoma:
- Least common, but has the worst prognosis
- Shows cavitations
SCLC vs NSCLC
| SCLC | NSCLC | |
|---|---|---|
| Cytoplasm | Scant | Abundant |
| Nuclei | Small and hyperchromatic with fine chromatin pattern | Pleomorphic with coarse chromatin pattern |
| Nucleoli | Indistinct | Prominent |
| Cells | In diffuse sheets | Glandular or squamous |
Clinical manifestations
- Local tumor growth:
- Central tumor with endobronchial growth:
- Cough
- Hemoptysis
- Wheeze and stridor
- Dyspnea
- Post-obstructive pneumonitis (fever and productive cough)
- Peripheral tumor with pleural involvement:
- Chest pain from pleural or chest wall involvement
- Dyspnea (restrictive)
- Symptoms of lung abscess (from tumor cavitation)
- Central tumor with endobronchial growth:
- Invasion or obstruction of adjacent structures:
- Tracheal obstruction
- Esophageal compression → dysphagia
- Recurrent laryngeal nerve paralysis → hoarseness
- Phrenic nerve paralysis → elevation of the hemidiaphragm and dyspnea
- Sympathetic nerve paralysis → Horner’s syndrome: enophthalmos, ptosis, miosis, and ipsilateral loss of sweating
- Malignant pleural effusion → dyspnea
- Pancoast’s (superior sulcus tumor) syndrome: from local extension of a tumor growing in the apex of the lung with involvement of the eighth cervical and first and second thoracic nerves → shoulder pain that characteristically radiates in the ulnar distribution of the arm
- Superior vena cava syndrome from vascular obstruction
- Pericardial and cardiac extension → tamponade, arrhythmia, or cardiac failure;
- Growth of regional lymph nodes through lymphatic spread
- Painless lymphadenopathy
- Lymphatic obstruction →pleural effusion
- Lymphangitic spread through the lungs with hypoxemia and dyspnea
- Growth in distant metastatic sites
- Brain: headache, nausea, neurologic deficits
- Bone: bone pain, pathologic fractures; bone marrow invasion with cytopenias or leukoerythroblastosis
- Liver: liver dysfunction, biliary obstruction, anorexia, and pain
- Lymph node: in the supraclavicular region and occasionally in the axilla and groin
- Spinal cord compression syndromes: from epidural or bone metastases
- Adrenal: common but rarely cause adrenal insufficiency
- Remote effects of tumor products (paraneoplastic syndromes)
- Paraneoplastic syndromes of unknown etiology: Present with systemic symptoms such as anorexia, cachexia, weight loss, fever, and suppressed immunity.
- Endocrine syndromes:
- Hypercalcemia and hypophosphatemia resulting from the ectopic production by squamous tumors of parathyroid hormone (PTH) or, more commonly, PTH-related peptide
- Hyponatremia with the syndrome of inappropriate secretion of antidiuretic hormone or atrial natriuretic factor by small cell cancer
- Ectopic secretion of ACTH by small cell cancer. ACTH secretion usually results in additional electrolyte disturbances, especially hypokalemia
- Skeletal–connective tissue syndromes: periostitis and clubbing
- Neurologic-myopathic syndromes:
- Lambert-Eaton myasthenic syndrome and retinal blindness in small cell cancer
- Peripheral neuropathies, subacute cerebellar degeneration, cortical degeneration, and polymyositis, seen in all lung cancer types
- Coagulation, thrombotic, or other hematologic manifestations:
- Migratory venous thrombophlebitis (Trousseau’s syndrome)
- Nonbacterial thrombotic endocarditis with arterial emboli
- Disseminated intravascular coagulation with hemorrhage
- Anemia
- Granulocytosis
- Leukoerythroblastosis
- Cutaneous manifestations: Rare; include dermatomyositis and acanthosis nigricans
- Renal manifestations: Rare; nephrotic syndrome and glomerulonephritis
Diagnosis
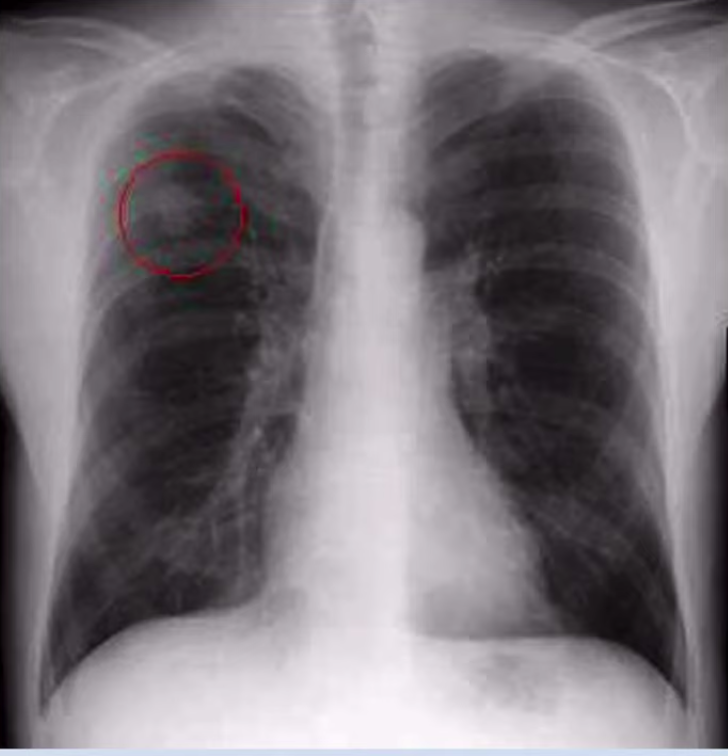
- Best initial test: Chest X-ray
- New lesion not seen on previous chest X-ray performed within the last two years is suspicious for cancer
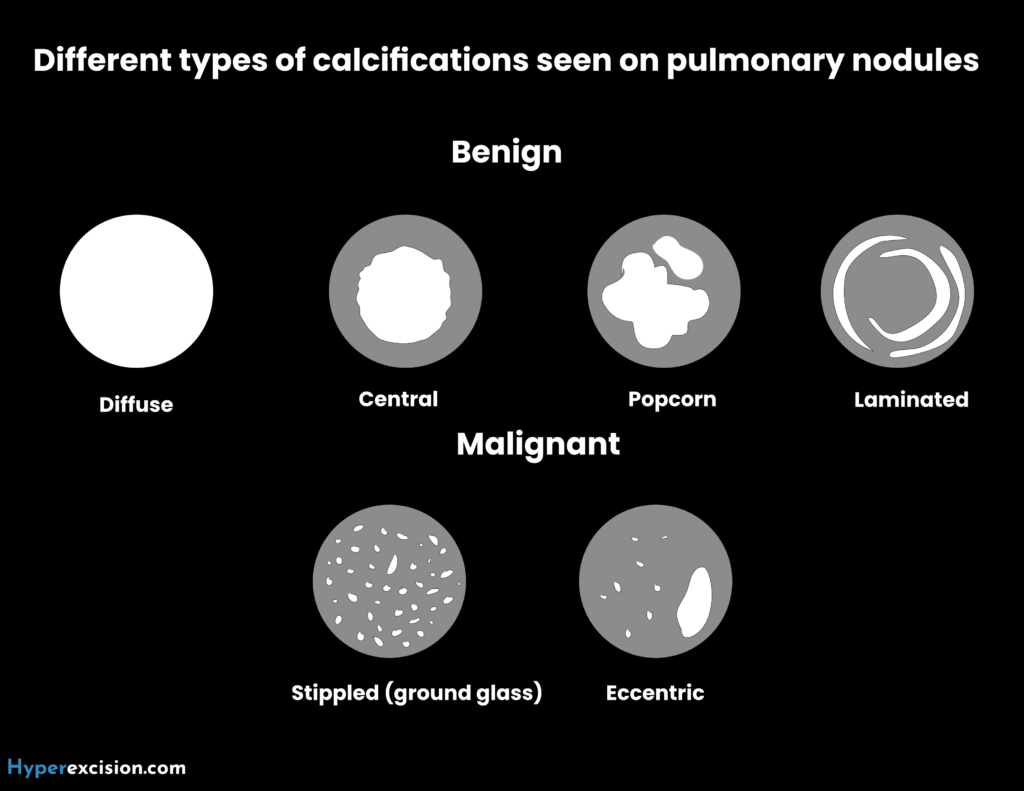
- A solitary pulmonary nodule (SPN) seen on chest X-ray could be benign or malignant
| Characteristics | Benign | Malignant |
|---|---|---|
| Size | <0.5 cm | >1 cm |
| Calcification | Uniform, concentric or popcorn | Noncalcified or nonuniform |
| Margins | Smooth | Irregular |
| Density | Dense and solid | Non-solid, ground-glass |
| Comparison | Seen on chest X-ray for >2 years | New or unknown lesion |
| Symptoms | Asymptomatic | Symptoms may be present |
- Most accurate test: Biopsy
- For peripheral lesions: Transthoracic biopsy, or video-assisted thorascopic surgery
- For central lesions: flexible bronchoscopy
- Upon diagnosis:
- Routine labs:
- CBC: Cytopenia→ Bone marrow metastasis
- Complete metabolic panel: electrolytes (SIADH), LDH (if elevated, worse prognosis), LFTs (if elevated, liver metastasis)
- Imaging:
- CT: staging
- Whole body MRI: check for metastasis
- Routine labs:
Management
- Mostly based on histological classification:
- SCLC: Chemotherapy with/ without radiotherapy
- NSCLC: Surgery with/ without radiotherapy
- Eligibility for surgery: pulmonary function tests are necessary. Best if FEV >2 L/s. Resections include wedge, segment, lobe, and unilateral pneumonectomy.
- Staging is required to determine optimum treatment.
- Surgical resection with curative intent is reserved in patients with early-stage disease. Adjunct therapy is used for more extensive disease.
Prevention
- Primary prevention: aimed mostly toward the younger population, to prevent them to start smoking
- For smoking addicts, various smoking cessation measures can be attempted.
Complications
Lung cancer has a SPHERE of complications
| Acronym | Complications |
|---|---|
| S | Superior vena cava syndrome |
| P | Pancoast tumor |
| H | Horner syndrome |
| E | Paraneoplastic |
| R | Recurrent Laryngeal Symptoms (Hoarsness) |
| E | Effusions (pleural or pericardial) |
Prognosis
- Patients’ 5-year survival rate is around 15%, and therefore lung cancer often has a poor prognosis.