A Fistula-in-ano is a communication between the anal canal and perianal skin. They are a notorious complication of perianal abscess and Crohn’s disease. It can occur at the site of a drain placement or at the incision used to drain the abscess. Fistula-in-ano can result in recurrent abscesses. Patients are often bothered by purulent or feculent drainage from the external opening. The location of the internal opening can be determined using Goodsall’s rule. Diagnosis is clinical.
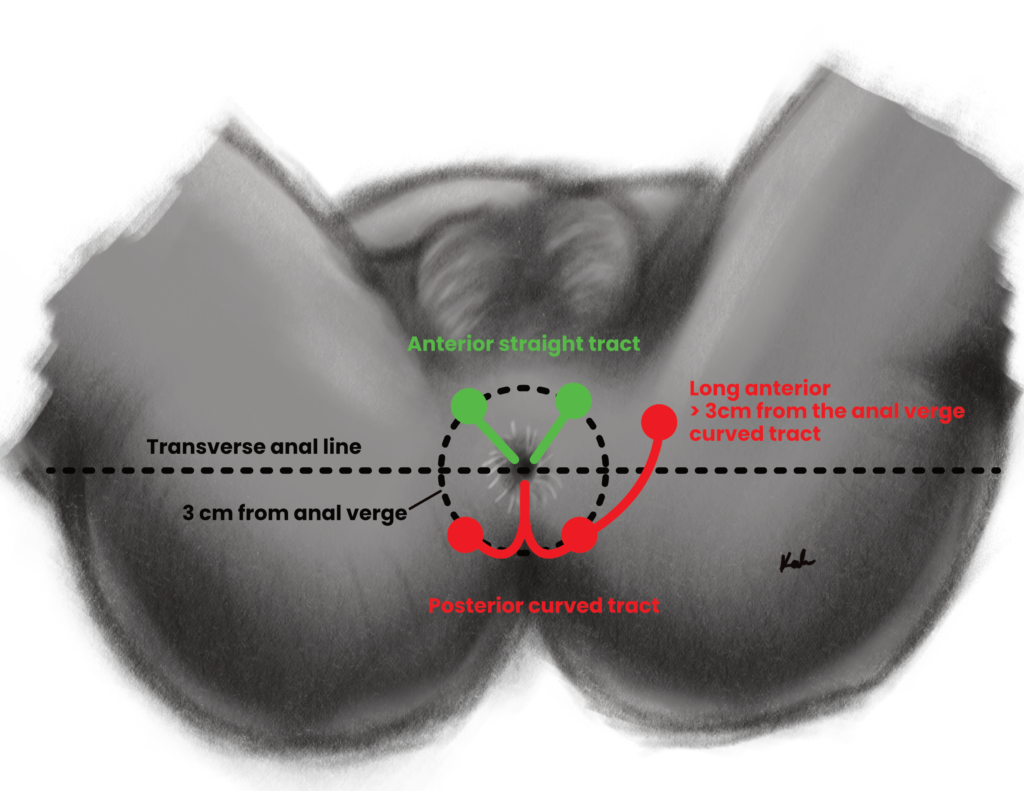
Goodsall’s rule for fistula in ano
Opening in relation to transverse anal line
Tract
Anterior opening
Travels in a radial (straight) path to the anal canal
Posterior opening
Travels in a curved tract to the anal canal. PC = Posterior opening takes a Convoluted course
Opening more than 3 cm from the anus
May travel in a curved tract to the anal canal
Goodsall’s rule for fistula in ano
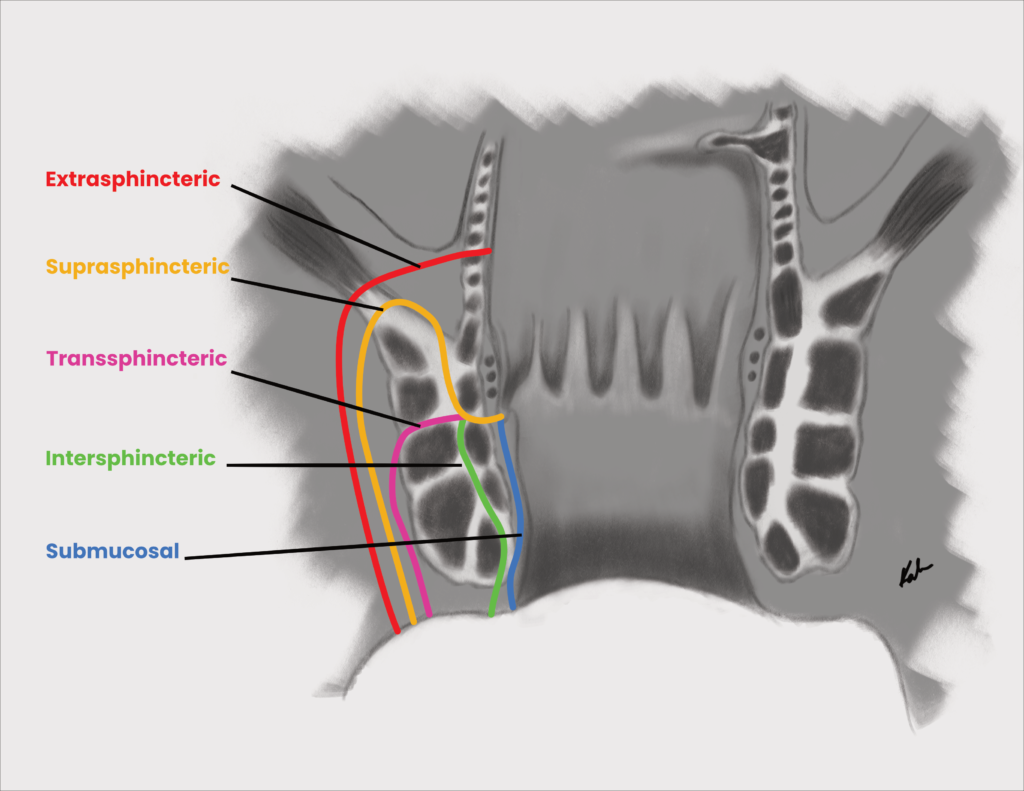
Classification of fistula in ano (Park’s)
Classification
Description
Intersphincteric
Penetrates internal sphincter to intersphincteric space
Transsphincteric
Penetrates internal and external sphincters to ischiorectal fossa
Suprasphincteric
Penetrates levator ani
Extrasphincteric
From the rectum above the dentate line through the levator ani
Signs and symptoms
Feculent or purulent peri-anal discharge
Perianal or rectal pain
Swelling
Bleeding
External opening visible
Investigations
Proctosigmoidoscopy or anoscopy under anaesthesia: for formal diagnosis
Treatment
Fistulotomy: cut along the length of the fistula to open it. Leave to heal by secondary intention.
Seton placement (cutting or draining): placed to keep the fistula tract open, ensure adequate drainage and fibrosis (healing). Cutting setons slowly divide the fistula while maintaining continence
Fibrin glue or fistula plug: provides scaffolding for collagen deposition,
Treat the underlying cause e.g. crohn’s disease
Antibiotics
Indications for fistulotomy
Intersphincteric and low transphincteric fistulas
Indications for seton placement
High transsphincteric, suprasphincteric and extrasphincteric fistula
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.