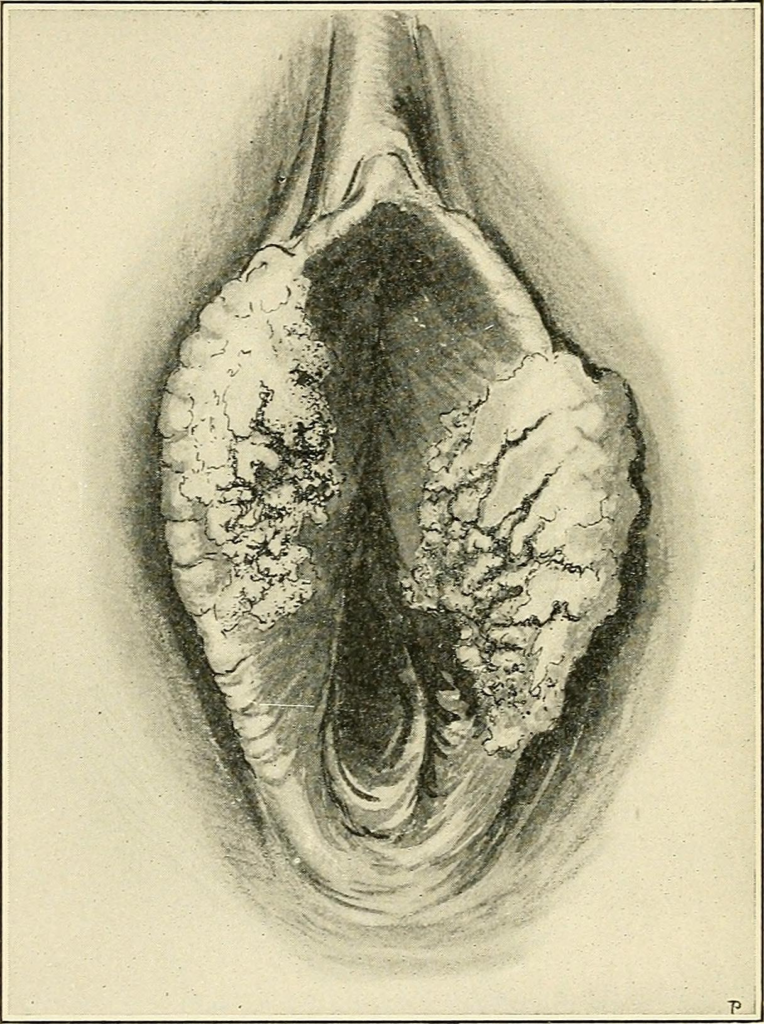
Vulvar carcinoma (squamous cell) can occur anywhere from the mons pubis to the perianal region. It is rare (3-5% of gynaecologic cancers). The incidence of Vulvar Carcinoma in Situ (VCIS) has increased by 411% between 1973 to 2000 due to increased HPV infection rates. The mean age of diagnosing vulvar cancer is 65 years. Vulvar Intraepithelial neoplasia is diagnosed at a younger age (39 – 50 years).
Classic Presentation of vulvar malignancy 4 P’s
Papule formation: Raised lesion +/- erosion and bleeding
Pruritic
Patriotic: Red, white, and blue in colour (similar to melanoma)
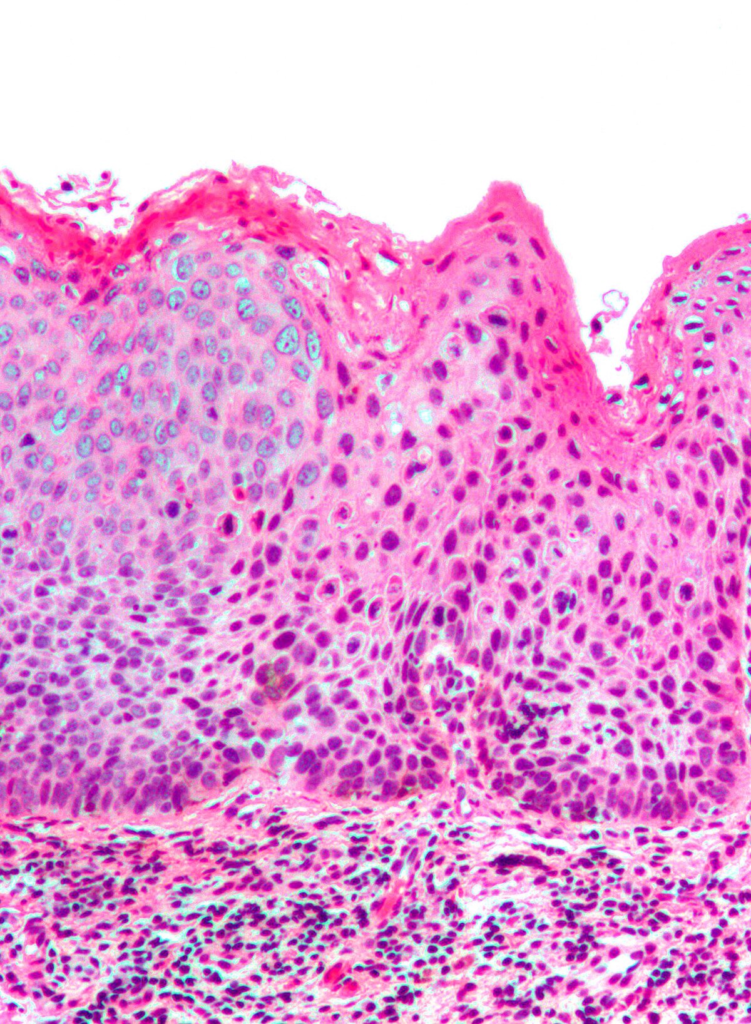
Parakeratosis: retention of nuclei in the stratum corneum
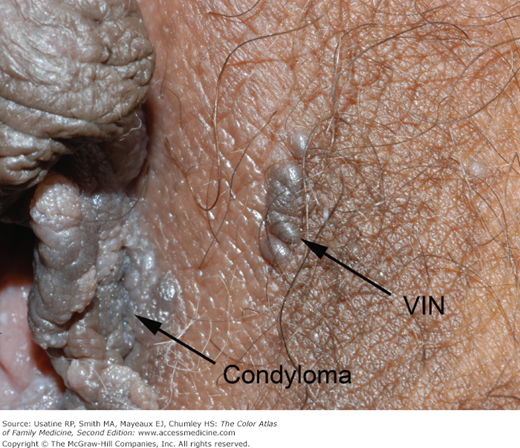
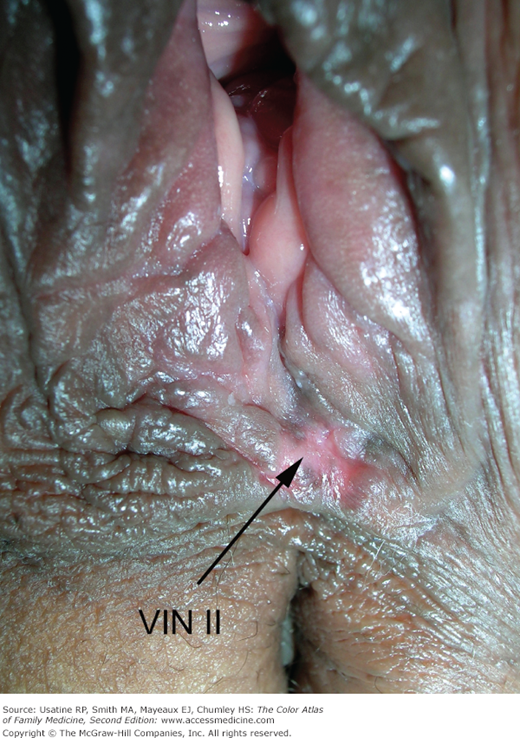
Vulvar Intraepithelial Neoplasia (VIN)
Vin is a premalignant change in the vulvar epithelium characterized by cellular atypia.
90% of vulvar cancers are squamous cell carcinomas. Typically presents as a pruritic, keratinized or pigmented, bleeding mass in a post-menopausal woman. Diagnosis is by punch biopsy obtained via vulvoscopy – the most abnormal-looking area is biopsied. Dyes are not necessary as in cervical malignancies.
Genital warts in an immunocompromised or post-menopausal woman
Genital warts that persist despite topical therapy (Podophyllin)
Evolving lesion (always suspicious for malignancy)
Treatment of VIN
If invasive cancer is suspected: Wide local excision
If invasive cancer is not suspected: Laser ablation
1986 ISSVD Classification
Classification
Description
VIN-1
Atypia in the deep 1/3 of the epithelium
VIN-2
Atypia in the deep 1/2 of the epithelium
VIN-3
Atypia in the deep 2/3 of the epithelium
VCIS
Full-thickness atypia confined to the basement membrane
2002 ISSVD Classification
VIN-1: eliminated because it was confirmed not to progress to vulvar carcinoma
VIN, usual type: strongly associated with HPV and smoking
VIN, differentiated type: less common, occurs in older women and is associated with lichen sclerosis and squamous cell hyperplasia. More likely to progress to SCC
Vulvar cancer is VIN + destruction of the basement membrane and invasion.
90% of vulvar cancers are SCC. Others include melanoma and Bartholin’s gland adenocarcinoma. The smaller the tumor the more likely the patient will be alive in five years.
Stage IB and II: Partial radical vulvectomy including ipsilateral inguinofemoral lymphadenectomy (bilateral lymphadenectomy should be performed if the tumor crosses midline)
Stage III: Radical vulvectomy including inguinofemoral lymphadenectomy. Followed by pelvic-groin irradiation +/- chemotherapy (Platinum based – Cisplatin/5-FU)
Stage IV: Radical vulvectomy including inguinofemoral lymphadenectomy. Occasional pelvic exenteration is done. Followed by chemoradiation
Staging of Vulvar cancer (TNM and Surgical)
1A can get wide local excision. 1B needs vulvectomy. Nodes to examine include the inguinofemoral nodes. Adjacent perineal structures include the lower 1/3 of the urethra, lower 1/3 of the vagina and anus.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.