Anatomy of the Vulva


Epidermal Inclusion Cyst
Epidermal inclusion cysts are caused by the proliferation of epidermal cells within a circumscribed area of the dermis which results in plugging of a pilosebaceous unit. It is AKA epidermoid cyst or sebaceous cyst. Usually an incidental finding on physical exam. Diagnosis is clinical.
- Patient History
- UV exposure
- HPV exposure
- Symptoms
- Most are asymptomatic
- Pain/Tenderness
- Odor and pus when infected
- Physical exam
- Flesh-colored cyst < 1cm in diameter
- Overlying erythema and tenderness if infected
- There may be cysts elsewhere
- Treatment
- Non-infected cyst:
- No management required
- Elective excision if patient finds it disfiguring
- Infected cyst:
- Incision and drainage
- Followed by anti-staph antibiotics (Dicloxacillin, Cephalexin)
- Non-infected cyst:
Hidradenoma
A hidradenoma is a benign cyst of the apocrine sweat gland. AKA apocrine hidradenoma or apocrine sweat gland cyst. Some patients may have a predilection towards abscess formation.
Hidradenitis suppurativa: a chronic disease characterized by recurrent hidradenomas with abscesses. Keloids may form following incision and drainage and hidradenomas may recur leading to chronic scarring. ****
Fox-Fordyce disease: a chronic disease characterized by recurrent non-infected hidradenomas. Worsened by exposure to heat and humidity
- Patient History
- Similar cysts elsewhere
- Symptoms
- Usually asymptomatic
- Physical exam
- Mobile 1-1.5cm nodule which may be ulcerated or inflamed
- Treatment
- Non-infected cysts
- No treatment required
- Elective excision if the patient finds it disfiguring
- Infected cysts
- Incision and drainage
- Followed by anti-staph antibiotics (e.g. Dicloxacillin, Cefalexin)
- Hidradenitis suppurativa
- Incision and drainage
- Long-term antibiotics (e.g. Doxycycline, Minocycline)
- Surgery for refractory cases (Laser and phototherapy, Radical surgery to remove the pilosebaceous unit)
- Non-infected cysts
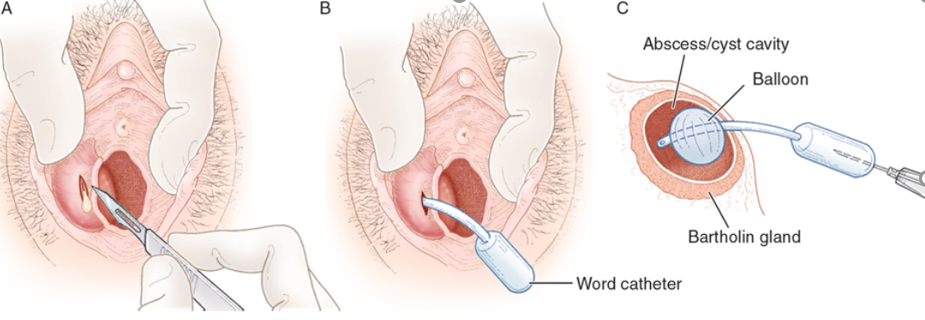
Bartholin Gland Cyst and Abscess
Bartholin cysts are caused by obstruction and cystic dilation of Bartholin’s duct. Diagnosis is clinical. Get a good sexual history to rule out chlamydia or gonococcal infection (chronic inflammation obstructs the orifice of the duct leading to cystic dilatation). Bartholin cysts in women over 40 years of age should be biopsied due to a small risk of Bartholin’s adenocarcinoma (a rare cause of vulvar carcinoma).
Bartholin’s glands are a paired set of glands found roughly at the 4 and 8 o’clock position of the vulva. They secrete mucus responsible for lubrication. Each gland is about 0.5 cm in size and drains into a duct 2.5 cm long. Ducts emerge onto the vestibule on either side of the vaginal orifice just inferior to the hymenal ring. They are homologous to the bulbourethral glands in males
- Patient history
- Reproductive age (commonly)
- History of trauma or non-specific infection
- History of chlamydia or Gonorrhea (in women with abscess)
- Symptoms
- Small cysts are asymptomatic
- Dyspareunia and Pain (for large cysts and abscesses)
- worsened with walking and sitting
- Physical exam
- Unilateral, round-ovoid cyst at the vaginal orifice
- Fluctuant or tense to palpation
- Distortion of vulvar symmetry in larger cysts
- Treatment
- Small, asymptomatic cysts
- No intervention is required (may regress on their own)
- Large, symptomatic cysts or abscesses
- Incision and Drainage
- Marsupialisation (Cut cyst and leave a big hole. More invasive, can damage nerves and lead to scarring) or
- Placement of a word-catheter
- Antibiotics post-I&D especially for women with confirmed Chlamydial or Gonococcal disease
- Small, asymptomatic cysts

Bartholin Gland Carcinoma
Rare adenocarcinoma. Most affected women do not have a history of Bartholin abscesses or cyst.
- Signs and symptoms
- Solid, cystic or abscesses
- Fixed on underlying tissue
- Solid area may be noted within cyst
- Painless vulvar mass
- Investigations
- Biopsy