Last updated:
April 1, 2026
Malnutrition is defined as a lack of macronutrients (calories) OR a lack of micronutrients (vitamins and minerals). Here, we will consider undernutrition in terms of inadequate consumption of macronutrients.
Anthropometric indices
| Indices | Description |
|---|---|
| Weight for age (W/A) | This is used to monitor growth in the child’s booklet. It cannot distinguish acute from chronic malnutrition. |
| Weight for height (W/H) or weight fo rlength (W/L) | This is the measure for acute malnutrition. A low W/H or W/L indicates wasting. |
| Height for age (H/A) | This is the measure for chronic malnutrition. A low H/A indicates stunting. |
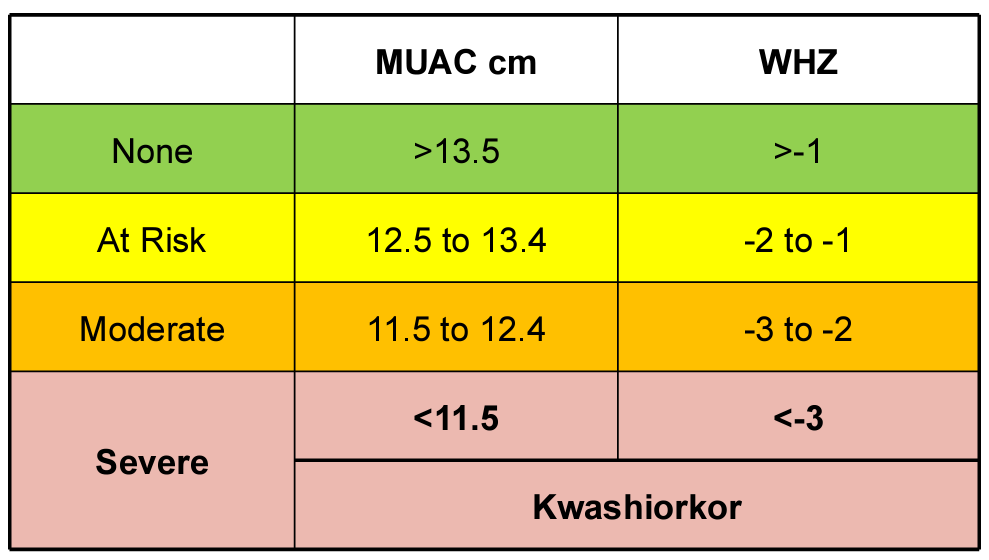
| Mid-upper arm circumference | Mid-upper arm circumference (MUAC) measurement using the Shakir tape is used to quickly assess nutritional status. It is used in children aged 6 months to 6 years |
BMI Scale – The BMI scale is used for adults, and to some extent, for children.
| BMI | Category |
|---|---|
| > 30 | Obese |
| 25 – 30 | Overweight |
| 18.5 – 25 | Normal |
| < 18.5 | Underweight |
Definition of terms
| Term | Description |
|---|---|
| Wasting | Weight for height (W/H) or weight for age (W/A) < 2 SD below the normal |
| Stunting | Height for age < 2 SD below the normal |
| Severe acute malnutrition (SAM) | SAM is defined as Severe wasting with a W/H < 3SD, or W/L <3SD, or MUAC <11.5, or gross severe wasting, or bilateral oedema without any other explainable cause |
| Protein-energy malnutrition (PEM) | The term Protein Energy Malnutrition is outdated. PEM refers to a life-threatening deficiency of macronutrients. It was defined by the WHO as a cellular imbalance between the supply of nutrients and energy and the body’s demand for them to ensure growth, maintenance and normal functioning. |
Wellcome-Trust Classification of Protein Energy Malnutrition
| Weight for age | Without oedema | With oedema |
|---|---|---|
| 60 – 80% | Underweight | Kwashiokor |
| < 60% | Marasmus | Marasmic Kwashiokor |
Differences between marasmus and kwashiorkor
| Marasmus (non-oedematous) | Kwashiokor (oedematous) | |
|---|---|---|
| General appearance | Weight loss, listlessness | Weight loss, lethargy, irritability |
| Skin | Loss of skin turgor and wrinkling, hypothermia | Edema and flabby skin tissue, dermatosis (hyper-pigmentation and desquamation – flaky paint dermatosis) |
| Facies | Simian facies | Moon facies |
| Volume status | Appears dehydrated | Appears volume overload |
| Gastrointestinal | Constipation or starvation diarrhoea | Diarrhoea and vomiting |
| Abdomen | The abdomen may be distended or flat | Distended abdomen +/- Hepatomegaly |
| Neuromusclular | Low muscle tone or hypotonia | Loss of muscle bulk |
Micronutrients of great concern in undernutrition
| Micronutrient | Importance |
|---|---|
| Zinc | Important during the rehydration and refeeding process. Urinary zinc is proportional to the overall zinc status |
| Iodine | Deficiency results in goiterous hypothyroidism and developmental issues (particularly in cognition) |
| Vitamin A | Deficiency causes night blindness, keratinous changes of the cornea, conjunctivae, skin and increased susceptibility to GI infections |
| Iron | Deficiency causes reduced synthesis of heme → microcytic anemia |
| Folic acid | Deficiency causes megaloblastic anaemia |
Clinical features of severe acute malnutrition
| System / Feature | Clinical Findings | Underlying Mechanism / Cause |
|---|---|---|
| Skin changes | Ulcerations | Zinc deficiency |
| Excessive dryness | Atrophy of sweat and sebaceous glands | |
| Hyperpigmentation, erythema, duskiness (exposed areas) | Niacin deficiency | |
| Cracking and fissuring | Nutritional deficiencies | |
| Generalized hypopigmentation | Skin stretching due to oedema | |
| Hair changes | Brittle hair | Impaired keratin synthesis (↓ cysteine & methionine) |
| Reddish/grey discolouration | Tyrosine deficiency | |
| Dull, lack of lustre | Withering of the hair cuticle | |
| Oedema | Generalized oedema | Hypoalbuminemia → ↓ oncotic pressure |
| RAAS activation due to hypovolemia | ||
| Pump malfunction → vascular leak | ||
| Free radical damage to membranes | ||
| Diarrhoea | Persistent/recurrent diarrhoea | ↓ secretory IgA, ↓ gastric acid |
| Pancreatic enzyme deficiency → malabsorption | ||
| Villous atrophy | ||
| Disaccharidase (lactase) deficiency | ||
| Candida albicans overgrowth | ||
| Recurrent infections | Frequent infections | Thymo-lymphatic atrophy |
| ↓ phagocytosis & bactericidal activity | ||
| ↓ complement and cytokines | ||
| Hypoglycaemia | Low blood glucose | Severe infection |
| Prolonged fasting (4–6 hours) | ||
| Anaemia | Pallor | Iron & folate deficiency |
| Parasitic infection (Necator americanus, Ancylostoma duodenale) | ||
| Malabsorption (chronic diarrhoea) | ||
| ↓ protein intake/synthesis | ||
| Apathy | Lethargy, reduced activity | Hypokalemia → muscle weakness |
| Mental slowing | ||
| Consequences of infection | Poor appetite | Illness effect |
| Dietary restriction | Misconceptions (e.g., reduced feeding during diarrhoea) | |
| Malabsorption | Gut dysfunction | |
| Protein-losing enteropathy | e.g., measles, HIV | |
| Vicious cycle | Infection ↔ malnutrition | |
| Zinc deficiency effects | Reduced appetite | Direct effect |
| Reduced immunity | Impaired immune function | |
| Prolonged diarrhoea | Impaired GI repair | |
| Poor weight gain | Even with adequate feeding | |
| Copper deficiency effects | Anaemia | Impaired iron metabolism |
| Poor bone growth | Defective collagen formation | |
| Selenium deficiency effects | Cardiac dysfunction | Impaired myocardial function |
| Renal function changes | ↓ GFR, ↓ renal plasma flow | Dehydration |
| Aminoaciduria | Tubular dysfunction | |
| ↓ acid excretion | Metabolic imbalance | |
| Poor urine concentration | Tubular impairment | |
| ↓ urea, ↑ Na⁺ & water retention | Altered renal handling | |
| Electrolyte imbalance | Hypokalemia, ↑ total body water | Na⁺/K⁺ pump dysfunction (energy-saving mode) |
| Liver | Hepatomegaly | Fatty liver |
Dermatitis in children with malnutrition
| Feature | Flaky Paint Dermatitis | Crazy Paint Dermatitis |
|---|---|---|
| Appearance | Large, dark, peeling patches, like flaking paint | Patchy, scaly, cracked skin, like a mosaic |
| Peeling pattern | In large sheets | Irregular and scaly |
| Location | Flexural areas (groin, axillae, buttocks) | Limbs and trunk |
| Cause | Severe protein deficiency | Micronutrient deficiencies (zinc, vitamin A, essential fatty acids) |
| Complications | Superimposed fungal/bacterial infections | Ulceration, secondary infections |
- Risk factors for severe acute malnutrition
- Poverty
- Single mothers
- Single parents
- Displacement by clashes
- Birth out of wedlock
- Mother and child are staying separate from father due to working conditions
- Sharing of income with extended families
- Precipitating factors for severe acute malnutrition
- Lack of food
- Famine
- Poverty
- Inadequate breastfeeding
- Wrong concepts about nutrition
- Diarrhoea and malabsorption
- Infections with worms, measles, or TB
- Lack of food
- Investigations
- Complete blood count: look for anemia due to Iron deficiency, folate/B12 deficiency (transfuse if Hb < 4mg/dL); Signs of infection
- Random Blood Sugar: look for hypoglycemia (cut-off at 3 mmol/L)
- U/E/C: look for electrolyte disturbances.
- TFTs: look for iodine deficiency
- Liver Function Tests: for albumin, BILIRUBIN
- Total protein: usually low
- Stool studies: ova and cysts. Antigens for rotavirus and adenovirus
- Other labs, as indicated by individual patient status (history/symptoms/physical exam)
- Complications
- Premature death
- This is the most immediate consequence of malnutrition
- Hypthermia
- Dehydration due to vomiting and diarrhoea
- Anaemia
- Infection
- Hypoglycaemia
- Premature death
- Treatment – stabilisation phase (week 1)
- Correct hypoglycemia: Defined as a blood glucose of < 3mmol/L
- Signs of hypoglycaemia include low body temperature (< 36.5 C), lethargy, and loss of consciousness. Sweating and pallor do not usually occur in children who are malnourished
- Correct hypothermia: Defined as axillary temp <35 C
- Correct dehydration: Can be treated with IV RLD5 or ReSOMAL. Whole blood or pRBC can be used if the child has anaemia (Hb < 4 g/dL)
- Correct electrolyte imbalances: use commercial F75 OR mineral mix and 4mmol/kg/day of potassium added to feeds. Do frequent electrolyte checks.
- Antibiotics for any suspected infection: IV Penicillin (or Ampicillin) and Gentamicin, Nystatin/Clotrimazole for oral thrush, Albendazole after 7 days of treatment. TEO (+ Atropine) for pus/ulceration in the eyes
- Correct micronutrient deficiency: Vitamin A PO if eye signs on admission and days 2 and 14, if no RUTF or F75/F100, give Multivits for at least 2 weeks, Folic acid 2.5mg for alternate days. Give Iron only when the child is gaining weight and no RUTF.
- Begin cautious feeding: F75 3 hourly for at least 7 days. (130mls/kg/day, 100mls/kg/day if severe edema or face)
- Achieve catch-up growth: F100 or RUTF 8 hourly. They are very high in energy and protein.
- Provide sensory stimulation and emotional support
- Prepare for follow-up after recovery
- Correct hypoglycemia: Defined as a blood glucose of < 3mmol/L
- Treatment – rehabilitation phase (week 2 – 6)
- Continue Nutrition: F100 or RUTF diet (100 kcal/kg/d)
- Iron replacement
- Factors for poor prognosis
- Serum albumin < 1g/dL
- Total bilirubin > 6 mg%
- Serum sodium < 120 mmol/L
Phases of treatment – treatment is phased to prevent refeeding syndrome
| Phase | Duration | Nota bene |
|---|---|---|
| Stabilization | 1 – 7 days | During the stabilization phase, start with smaller and more frequent feeds before phasing up to larger and less frequent feeds as tolerated. |
| Rehabilitation | Week 2 – 6 | |
| Followup | Week 7 and beyond |
Differences between ReSoMal and Standard ORS
| Feature | ReSoMal (Rehydration Solution for Malnutrition) | Standard ORS (Oral Rehydration Solution) |
|---|---|---|
| Purpose | Specifically for dehydration in Severe Acute Malnutrition (SAM) | General dehydration due to diarrhea, including cholera |
| Sodium (Na⁺) | 45 mmol/L (lower to prevent sodium overload and worsening edema) | 75 mmol/L (higher, which can cause fluid overload in SAM) |
| Potassium (K⁺) | 40 mmol/L (higher to correct SAM-related potassium deficiency) | 20 mmol/L (lower, insufficient for SAM) |
| Magnesium (Mg²⁺) | 3 mmol/L (included to correct deficiencies common in SAM) | None (not designed for SAM) |
| Zinc (Zn²⁺) | Added (supports immune function and gut healing) | May or may not contain zinc, depending on formulation |
| Glucose | Reduced (to lower osmolality and avoid worsening diarrhea) | Higher (can worsen osmotic diarrhea in SAM) |
| Osmolality | Lower (~300 mOsm/L) to prevent osmotic diarrhea | Higher (~310–345 mOsm/L), which may worsen diarrhea in SAM |
| Edema Risk | Low (prevents sodium overload and worsening edema) | High (excess sodium can worsen edema in SAM) |
| Use in SAM | Preferred | Not recommended (unless ReSoMal is unavailable, in which case ORS must be diluted) |
| Use in Cholera or Severe Dehydration | Not recommended (does not replace fluids lost in cholera) | Recommended (high sodium content matches cholera-related fluid loss) |
Difference between F-75 and F100
| Feature | F-75 (Stabilisation Phase) | F-100 (Rehabilitation Phase) |
|---|---|---|
| Purpose | Initial stabilisation and metabolic recovery | Rapid weight gain and catch-up growth |
| Energy | 75 kcal per 100 mL | 100 kcal per 100 mL |
| Protein | 0.9 g per 100 mL | 2.9 g per 100 mL |
| Fat | 1.9 g per 100 mL | 5.3 g per 100 mL |
| Carbohydrates | 9.3 g per 100 mL | 10.5 g per 100 mL |
| Osmolality | Low (prevents osmotic diarrhea) | Higher |
| Iron Content | No iron (to avoid fueling infections) | Contains iron |
| Use | Stabilisation phase (first 3–7 days) | Rehabilitation phase (once appetite returns and weight gain begins) |