Introduction
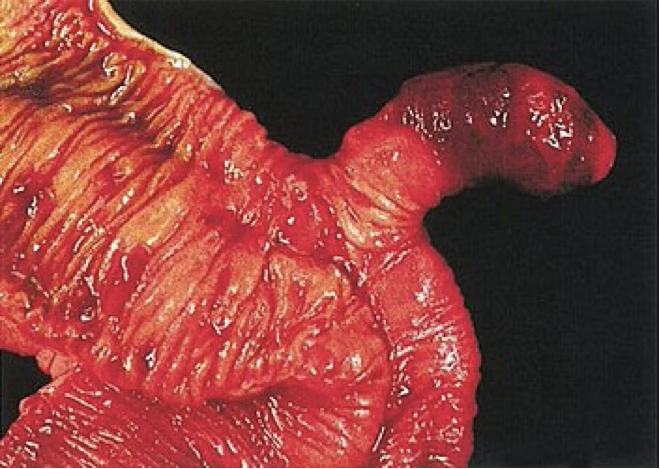
Meckel’s diverticulum is a blind out-pouching of anti-mesenteric aspect of the middle-to-distal ileum. It is a true diverticulum of the gastrointestinal duct containing all layers of the bowel walls and its own artery.
It is named after Johann Friedrick Meckel, the Younger (1781-1833).
A Meckel’s diverticulum may contain gastric, pancreatic, liver, carcinoid or lymphatic tissue, which predispose to the production of complications.
It is primarily a paediatric disease but can occur in adults (with a different set of symptoms).
Embryology
Meckel’s diverticulum is due to a persistence of the vitello-intestinal tract (a vestigeal remnant). The omphalomesenteric/ vitelline/ vitello-intestinal duct is a tubular structure connecting alimentary canal to yolk sac in embryonic life, normally obliterated by 5-7th week.
Incomplete obliteration → persistence of proximal intestinal segment of duct → Meckel diverticulum. Free in 75% of cases, however may be connected to navel by fibrous cord (obliterated part of duct).
Blood supply – Vitelline artery; branch of SMA, crosses over ileum to supply diverticulum. Normally obliterated by 9th week.
- Vitelline cord – Persistence of tract, obliteration of lumen
- Umbilicoileal/ Vitelline fistula – Persistence and patency of entire tract
- Vitelline cyst/ Enterocyst – Persistence of central portion of duct, ends obliterate
- Meckel diverticulum
- Meckel diverticulum with vitelline cord – Free in 75%
- Vitelline/ Umbilical sinus – persistence of duct at umbilical end, ileal end obliterates
Rule of 2s in Meckel’s diverticulum
- Affects ≈2% of the population (Most common congenital anomaly of the GIT)
- ♂:♀ 2:1 (occurrence equal but complications hence diagnosis more common in ♂)
- Commonly diagnosed before 2 years of age
- 2 inches long, 2cm wide
- 2 feet proximal to ileocecal valve
- ≈2% become symptomatic
- 2 types of mucosa:
- Native ileal mucosa
- Ectopic mucosa: (≈60% gastric, ≈6% pancreatic, others e.g. jejunal, colonic, rectal, hepatobiliary)
Clinical features of a Meckel’s diverticulum
| Clinical feature | Description |
|---|---|
| Haemorrhage (Lower GI bleeding) | Due to peptic ulceration in the presence of gastric mucosa. Presents as painless hematochezia in children and melaena in adults. Most common presentation in children. |
| Intestinal obstruction | Due to volvulus around the diverticulum, intussusception, strictures, Littre’s hernia, direct obstruction by a fibrous band connecting the apex of the diverticulum to the umbilicus. Most common presentation in older children and adults. |
| Meckel’s diverticulitis | Abdominal pain with a similar presentation to appendicitis (RLQ pain, fever, tenderness, leukocytosis). Perforation presentation similar to perforated duodenal ulcer. |
| Chronic ulceration | Presents with peri-umbilical pain |
| Perforation/ Peritonitis | Presentation with acute abdomen, resulting from severe diverticulitis or peptic ulceration |
| Littre’s hernia | Diverticulum is present in an inguinal or femoral hernia |
- Signs and symptoms in children
- Painless haematochezia (due to fast intestinal transit time)
- Maroon coloured stool
- Signs and symptoms in adults
- Melaena (due to slow gastrointestinal transit time)
- Crampy abdominal pain
Diagnosis
- Evaluate LGIB
- Stool guiac test: Positive
- Nasogastric tube aspirate: no blood lavaged
- Esophagogastruoduodenoscopy: no source of bleeding
- Evaluate acute abdomen
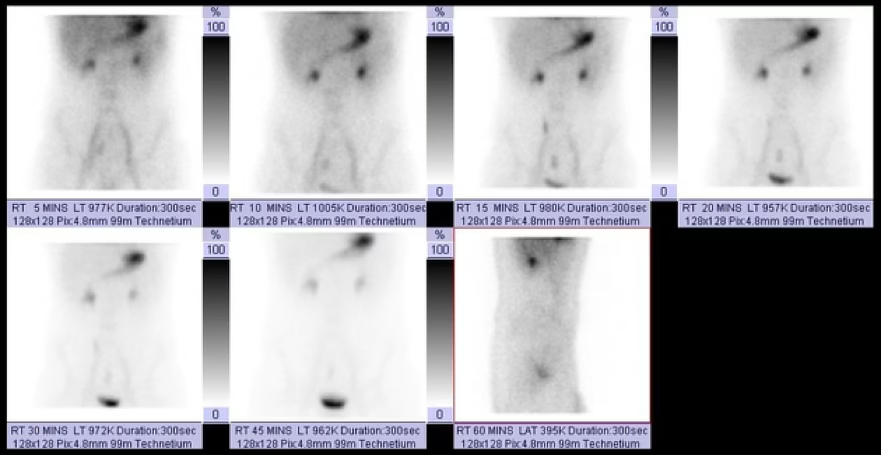
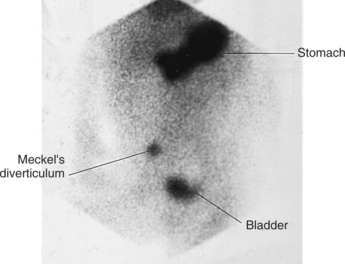
- Imaging
- Meckel scan (T-99 scintigraphy) – Technetium-99m pertechnetate scan to detect gastric mucosa
- Abdominal U/S – intussusception, inflamed diverticula
- CT angiography – localize source of bleed, patent vitelline artery pathognomonic
- CT or MRI with contrast – r/o ddx e.g. appendicitis or diagnose complications e.g. IO
- Endoscopy – Double-balloon enteroscopy or capsule endoscopy
Management
Asymptomatic patients
Detected incidentally on imaging/surgery
- Resection in children, do not resect >50yrs
- In adults <50 years consider resection if: male, palpable, longer than 2cm, broad base >2cm, signs of ectopic tissue
Symptomatic patients
- Stabilize: ABCDEs
- IO: NGT, NBM, IV fluids
- GIB: start PPIs, OGD, colonoscopy
- Definitive: open/ laparoscopic surgery
- Broad base: Bowel resection (wedge ileal resection with anastomosis)
- Narrow base: Meckel’s diverticulectomy (resection of diverticulum)
- Stapling of the diverticulum to prevent pepsin from entering ileum
Clinical scenario
A mother brings her 3-year-old child into the casualty department due to increasing fatigue and reduced appetite over the past month. He has no history of fever, vomiting, abdominal pain or frank blood in stool. Has occasional dark sticky stools that his mother thought were due to previously prescribed iron supplements. He is pale on examination, with stable vitals and a small amount of melena stool on DRE. Complete blood count showed a microcytic hypochromic picture. Stool occult blood test was positive. Upper endoscopy and colonoscopy were normal. What is the most likely diagnosis?
- Intussusception
- Duodenal ulcer
- Adhesions
- Meckel Diverticulum
- Ulcerative Colitis
References:
Llewellyn KJ, Knaggs M, Serena T, Gerken JR. Concurrent Appendicitis and Meckel’s Diverticulitis Presenting With Small Bowel Obstruction in an Adult: A Case Report. Cureus. 2024 Aug 16 [cited 2025 Jul 17]; Available from: https://www.cureus.com/articles/266675-concurrent-appendicitis-and-meckels-diverticulitis-presenting-with-small-bowel-obstruction-in-an-adult-a-case-report UFO Themes. Pediatric Abdomen. Basicmedical Key. 2017. Available from: https://basicmedicalkey.com/pediatric-abdomen/ Nafisa K Kuwajerwala, MD. Meckel Diverticulum: Background, Anomalies of Omphalomesenteric Duct, Complications of Meckel Diverticulum. Medscape.com. Medscape; 2023. Available from: https://emedicine.medscape.com/article/194776-overview#a2 Pérez Domínguez R, Candia G, Alejandro Santilli H, Schlain S. Complicated Meckel’s diverticulum. Fifteen Years of Experience in an Interzonal Hospital in the Province of Buenos Aires. Revistasacp.com. 2022. Available from: https://revistasacp.com/index.php/revista/article/download/235/532?inline=1