Macular degeneration is the most common cause of permanent visual loss in the elderly. It is AKA age-related macular degeneration (AMD). It is a chronic condition that leads to progressive ventral visual loss. The macula is essential for central vision. Degeneration therefore leads to visual disruption causing distortion (metamorphopsia) and loss of central vision (central scotomas).
Its etiology is unknown. It typically presents as an older patient with blurry vision and dark spots that worsen over time. All patients with AMD receive regular followup with optometry. No effective surgical or medical treatment currently exists for dry AMD.
Type of AMD
Features
Frequency
Progession of symptoms
Dry (geographic) AMD
Associated with drusen (yellow cholesterol-based debris) between the RPE and choroid
80%
Slowly progressive
Wet (exudative) AMD
Associated with neovascularization of the choroid, leading to hemorrhage, ischemia, and scarring. It is more severe and progressive
10-15%
Rapidly progressive (over days or weeks)
Important relevant anatomy:
Bruch’s membrane
Innermost layer of the choroid located beneath the retina
Retinal pigment epithelium
Located in the retina beneath the photoreceptors next to the choroid (Bruch’s membrane)
Dramatic decrease in visual acuity (affects the ability to read and distinguish faces)
Decreased contrast sensitivity
Investigations
Ophthalmoscopy (indirect and dilated): for definitive diagnosis and differentiation (wet or dry AMD)
Snellen chart
Reduced visual acuity compared to the previous test
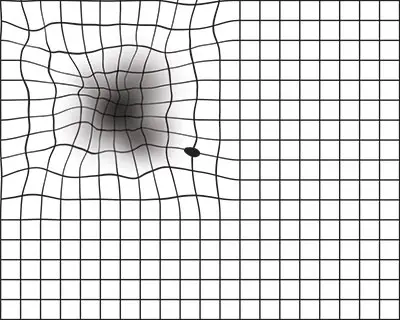
Amsler grid
Distortion
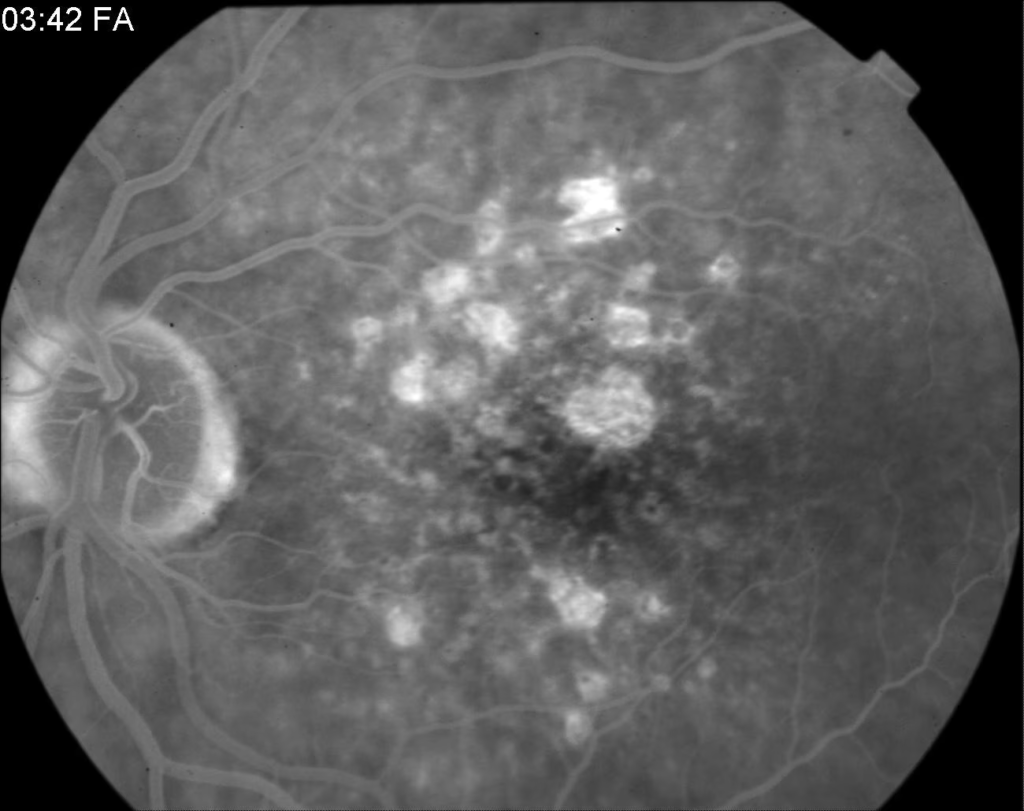
Fluorescein angiography: performed in suspected wet AMD to visualize abnormal blood vessels
Areas of bleeding (bright spots) around the macula
How Amsler grid may appear in a patient with AMD. Source- American Academy of Ophthalmologists
Dry Macular Degeneration
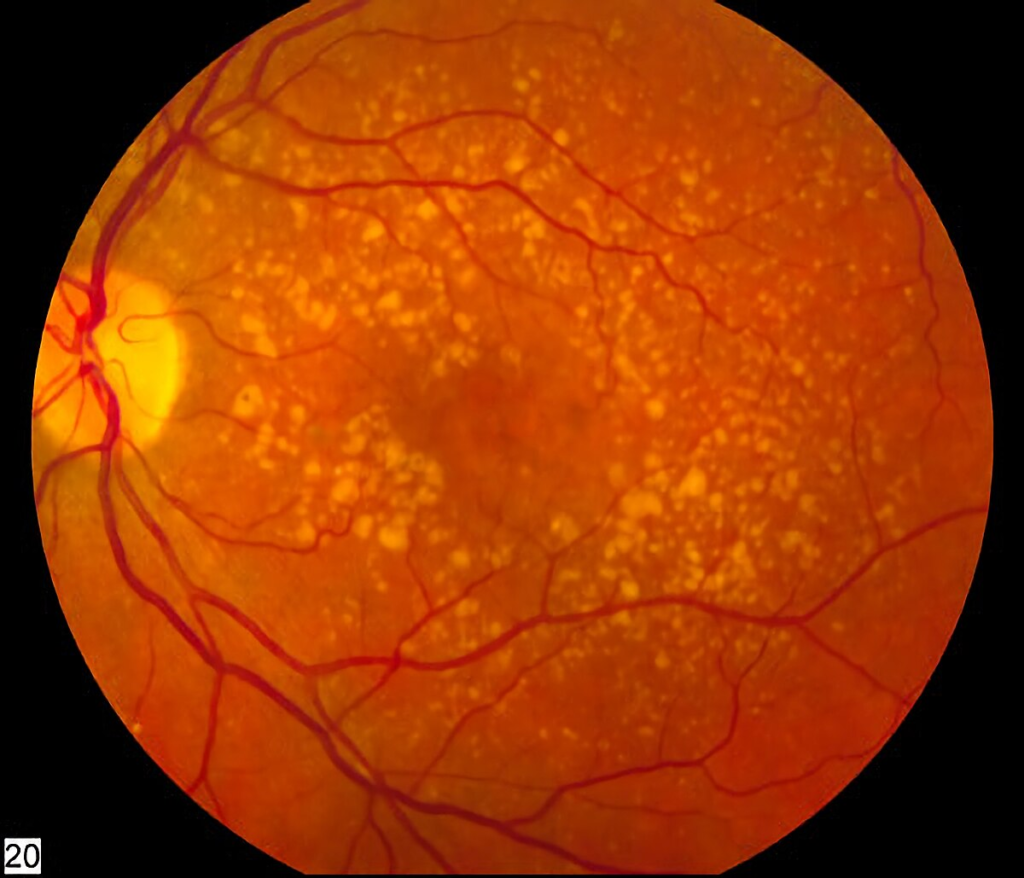
This is as a result of the accumulation of drusen. Drusen is yellow extracellular material that forms between Bruch’s membrane and retinal pigment epithelium (RPE). It results in gradual loss of vision. There is no specific treatment. Vitamins and antioxidant supplements may prevent it.
Drusen seen overlying the macula in dry AMD
Drusen is a common finding. The presence of drusen is not pathognomonic for AMD. However, the more drusen the more likely the patient will develop AMD.
Fluorescein angiography showing hyperfluorescence where there is atrophy of the RPE. Source- Medscape
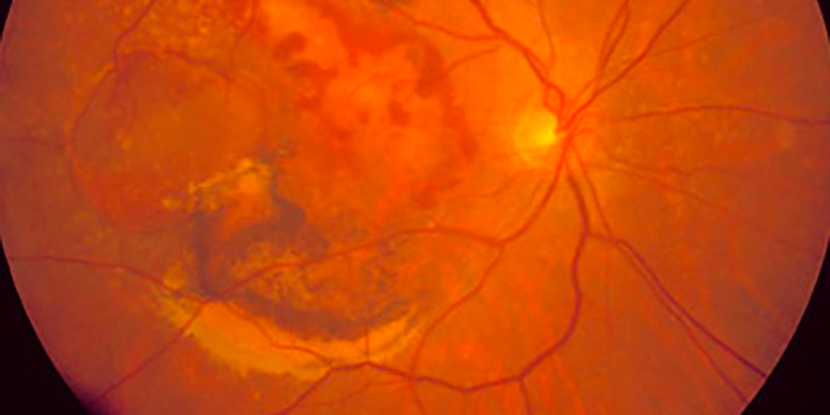
Wet Macular Degeneration
This is caused by a break in Bruch’s membrane. Blood vessels form beneath the retina which later leak and cause haemorrhage. It can progress rapidly to vision loss. Treatments include laser therapy and anti-VEGF medication (e.g. ranibizumab).
Treatment summary
Dry AMD
Refer to an optometrist to facilitate care and improve quality of life
Oral vitamins and anti-oxidants: slows progression
Wet AMD
Photodynamic therapy (PDT): lasers are used to coagulate abnormal vessels and slow the progression
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.