Anatomy of the Knee Joint
The knee is a modified hinge joint that articulates the femur to the patella and tibia. It is ‘modified’ because it allows for some degree of internal and external rotation, in addition to flexion and extension.
**https://youtu.be/_q-Jxj5sT0g**
Medial Collateral Ligament (MCL) tear
The MCL (tibial collateral ligament) is the most frequently injured knee ligament. MCL injuries are often associated with medial meniscal injuries and sometimes ACL injuries (”unhappy triad”). Diagnosis is clinical but MRI is obtained for formal diagnosis.
- Mechanism
- Excess valgus stress: Lateral blow or momentum to the knee in a fixed position
- MCL takes damage because it is stretched when the knee is pushed in (valgus pressure)
- Signs and symptoms
- Swelling and bruising along the course of the MCL
- Point tenderness over the medial joint line
- Positive valgus stress test
- Investigations
- MRI: most accurate test
- Non-operative treatment
- Immobilization with a hinged cast (for isolated injury)
- Rest or activity modification
- Operative treatment
- Surgical repair (for multiple or severe injuries)
**https://youtu.be/xNPLMfYXpVQ**
Lateral Collateral Ligament (LCL) tear
LCL (fibular colateral ligament) tears are less common than MCL tears. They are nearly always managed operatively.
- Mechanism
- Medial blow or momentum to the knee while in fixed position
- Signs and symptoms
- Swelling
- Point tenderness over the lateral joint line
- Positive varus stress test
- Investigations
- MRI: the most accurate test
- Treatment
- Immobilization with a hinged cast (for isolated injury)
- Surgical repair (for multiple or severe injuries)
Anterior Cruciate Ligament (ACL) tear
ACL originates from the lateral femoral condyle and inserts on the anteromedial tibia. It provides restraint to anterior translation of the tibia and rotational stability. The ACL is weaker than the PCL and is more frequently injured. ACL tears are common in sudden cutting and stopping sports (football and basketball) or contact sports (rugby). A torn ACL alters knee movement which may lead to early degenerative changes and arthritis.
Patterns of ACL tear
| Pattern | Description |
|---|---|
| Isolated Ligament tear | Only the ACL is torn |
| Tibial spine fracture | Involves an avulsion at the tibial insertion |
| Segond fracture | Avulsion of the proximal lateral tibia by the anterolateral ligament associated with ACL tear |
- Mechanism
- Rotation of the femur while the leg is planted
- Non-contact injury: sudden stopping or pivoting on a flexed knee
- Contact injury: blow to the posterior knee with the leg in a fixed position
- Signs and symptoms
- Swelling and pain of the knee
- Instability of the knee (wobbly knee)
- Positive anterior drawer test
- Positive pivot shift test (rotational instability)
- Investigations
- Plain radiograph: may identify avulsion fractures
- MRI: most accurate test. The drawer tests is not as sensitive or specific
- Non-operative treatment
- Immobilization: for those that do not strenuously use the knee joint i.e. non-athletes
- Operative treatment
- Graft placement
- Autografts (patellar tendon, hamstrings tendon, or quadriceps tendon)
- Allograft from cadavers
- ACL repair is not done since it is likely to fail over time
- Graft placement
Posterior Cruiciate Ligament (PCL) tear
PCL originates from the anterolateral medical femoral condyl and inserts into the posterior tibial sulcus. It provides restraint to posterio translation of the tibia. The PCL is stronger than the ACL and is less ocmmonly torn. Injury frequently involves other ligaments, cartilaginous or bony structures of the knee.
- Mechanism
- Direct blow to the anterior knee with the leg in a fixed position
- Falling onto a bent knee
- Motor vehicle collision (when the knee is suddenly forcefully pushed backwards)
- Signs and symptoms
- Swelling and pain of the knee
- Instability of the knee
- Positive posterior drawer test
- Investigations
- Plain radiograph: rule out avulsion fracture
- MRI
- Treatment
- Immobilization (for non-athlete/isolated injuries)
- Operative repair (for combinaiton injuries or athletes)
Posterolateral Corner (PLC) injuries
The PLC is a collection of ligaments that provide lateral stability to the knee. The 3 most important ligaments in the PLC are the LCL, popliteus tendon, and polpiteal fibular ligament. Diagnosis is by MRI. Treatment may be non-operative or operative depending on the severity of injury, whether other ligaments are injured, and the activity level of the patient.
Meniscus tear
The medial and lateral menisci are crescent-shaped fibrocartilage that provide joint stability, shock absorption, load distribution and proprioception. The medial meniscus is less mobile than the lateral meniscus, is more oval in shape, and is more prone to injury. It has a higher risk of injury in ACL-deficient knees. The lateral meniscus is more mobile, C-shaped, and commonly torn with acute ACL tears. ****Injury occurs commonly during sports.
Blood flow to the menisci occur from peripheral to central zones
| Zone | Perfusion |
|---|---|
| Peripheral (red zone) | Vascularized and well perfused |
| Central third (white zone) | Avascular and poorly perfused. May impact healing. |
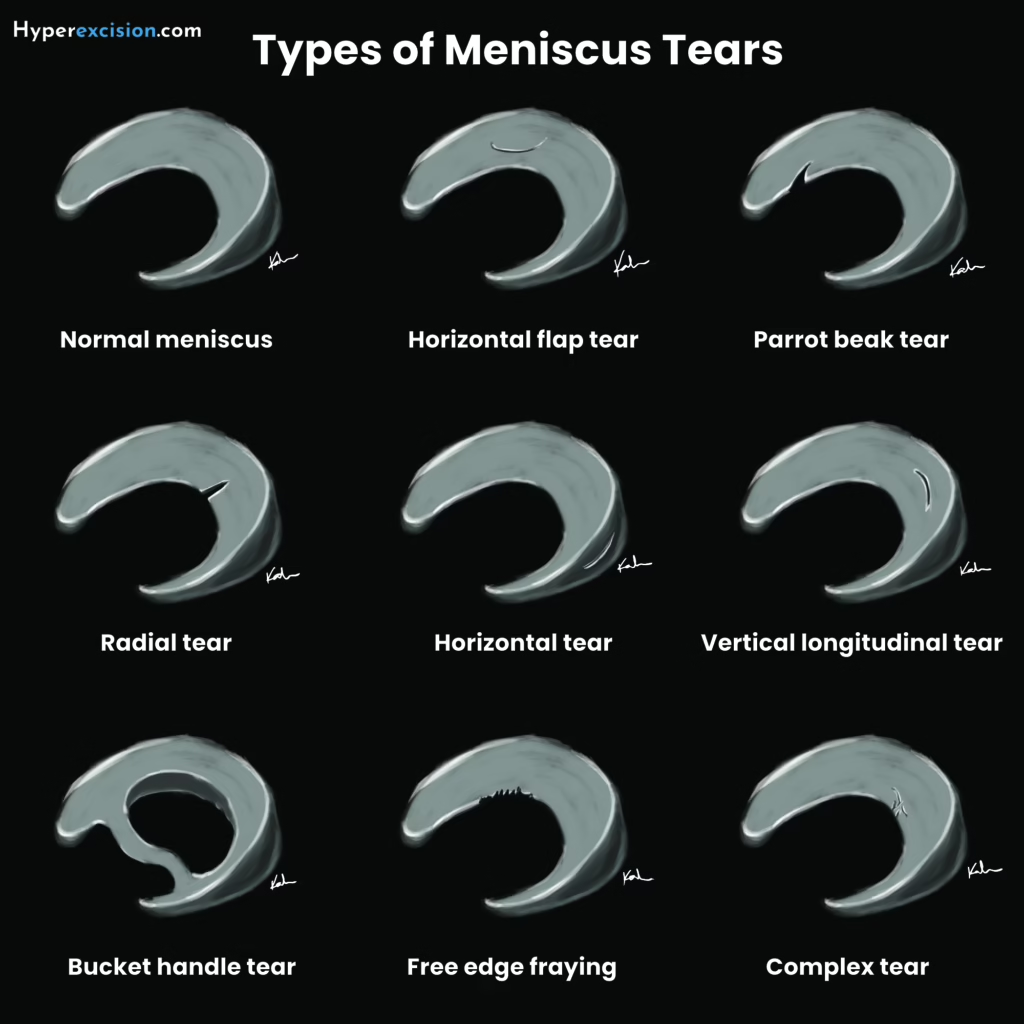
| Pattern of tear | Description |
|---|---|
| Vertical (longitudinal) | Common. Associated with ACL tears. Repaired if they are in a peripheral location |
| Bucket handle | Vertical tear that displces into the notch |
| Oblique (flap or bucket handle) | May cause mechanical locking symptoms |
| Radial | |
| Horizontal | More commoni n older populations. Associated with meniscal cysts |
| Complex | |
| Root | Latera root tears are associated with ACL tears. Medial root tears are associated with chondral injuries. |
- Mechanism
- Injury occurs often in sports
- Involves a sudden motion (contact or while squatting and twisting the knee)
- Associated with a “pop” or “click” experienced by the patient
- Signs and symptoms
- Protracted pain of the knee (will not get better with immobilization)
- Some swelling
- Tenderness at the joint line (most specific)
- “Clicking”
- Positive McMurray test
- Investigations
- Plain radiograph: to evaluate overall alignment and degenerative changes
- MRI: for diagnosis
- Operative treatment
- Arthroscopic repair of the meniscus
- Partial meniscectomy
- Meniscus transplant

Derrick Rose (Chicago Bulls #1) suffers a medial meniscus injury to his right knee. Note how the knee is flexed and twisted then wobbles before he moves on.
Knee dislocation
Knee dislocation are rare but an emergency when they happen. It occurs when three of the major ligaments are completely torn. The leg is present free floating from the thigh. It is associated with neurovascular compromise distal to the injury (since the popliteal artery is at high risk)
- Mechanism
- High energy trauma
- Signs and symptoms
- Pain
- Swelling
- Gross deformity present or reported by EMS (may spontaneously reduce prior to presentation)
- Assess pulses and ABI
- Investigations
- Ankle-Brachial Index
- Arteriography or duplex ultrasound over the popliteal artery: if ABI < 0.9
- X-ray of the knee joint after management
- Treatment
- Reduction
- Vascular surgery for possible revascularization