Add a header to begin generating the table of contents
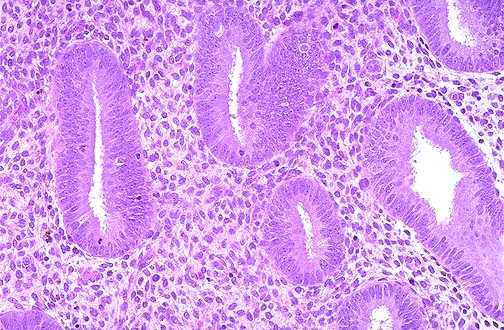
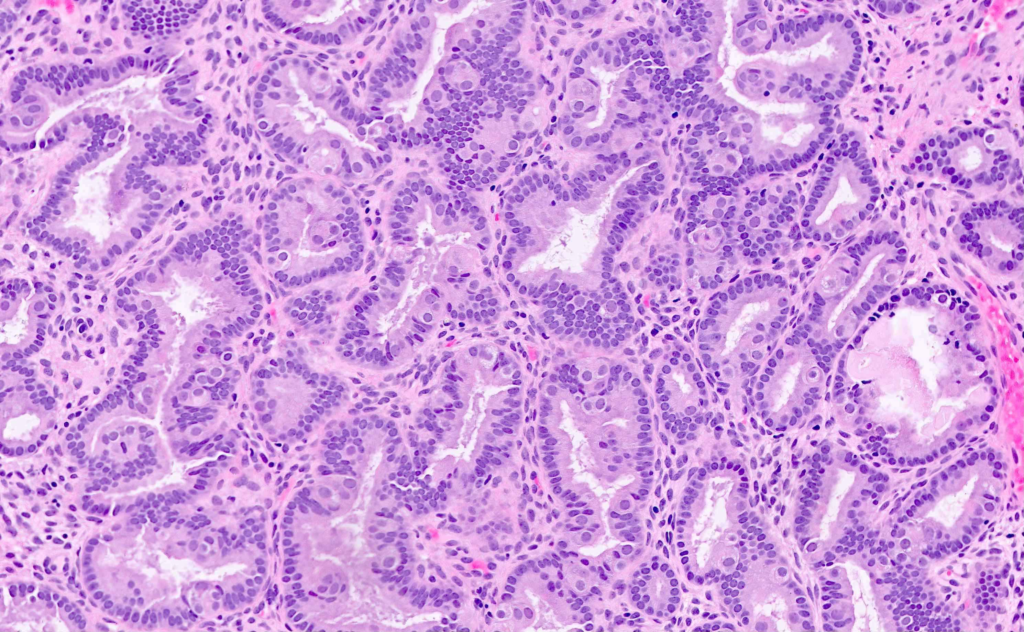
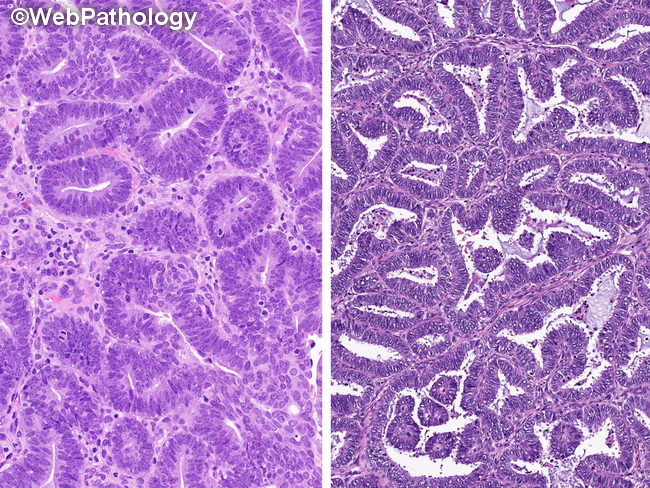
Endometrial hyperplasia is endometrial thickening with a proliferation of irregularly sized and shaped glands. Tends to be symptomatic in post-menopausal women. Endometrial hyperplasia in a post-menopausal woman (around 10mm) would be a normal endometrial thickness for a pre-menopausal woman in the secretory phase of her cycle. The class of hyperplasia is determined by histology. Endometrial tissue is extremely responsive to estrogen. Hyperplasia may be a precancerous lesion, although a majority do not develop into adenocarcinoma. Treatment depends on the age of the woman and whether or not there is atypia. MDPA or Megestrol is the medical treatment of choice.
1 in 38 women will develop endometrial cancer in their lifetime.
Risk factors
Hyperestrogenism (unopposed estrogen)
High-dose menopausal estrogens
Obesity (more aromatase more estrogen)
Nulliparity
Early menarche (≤ 11 years)
Late menopause
Use of Tamoxifen (SERM given for ER+ Breast cancer. Estrogen agonist in the uterus)
PCOS (anovulation → unopposed estrogen)
Type 2 diabetes, Hypertension, and Gallbladder Disease (may be independent, but occur more commonly in obese women)
White race
High socio-economic sttus
Older age
Living in North America or Northern Europe
Patient History
Use of post-menopausal estrogen supplements
Use of Tamoxifen
Nulliparity
Early onset of menarche and Late menopause
Family History of malignancies (Lynch syndrome etc.)
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.