Overview
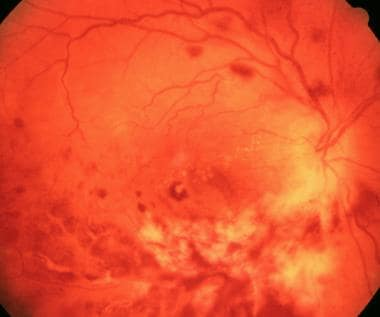
Retinitis occurs in conditions that cause retinal inflammation, resulting in edema and necrosis. Patients typically experience floaters (dark spots in the visual fields) and decreased vision. Infectious retinitis is usually a manifestation of systemic illness. Cytomegalovirus is a classic cause of retinitis. It is typically associated with immunocompromised patients (e.g. HIV/ AIDs patients with a CD4 count < 50, transplant patients on immunosuppression). It is crucial to rapidly diagnose and treat retinitis to decrease the risk of infection of the contralateral eye and blindness.
- Ocular signs and symptoms
- Blurry vision
- Floaters
- Symptoms consistent with retinal detachment (pain may or may not be present)
- Hallmark changes on fundoscopy
- Retinal haemorrhages
- Whitish appearance to the retina
CMV Retinitis
CMV causes retinitis in immunocompromised patients or through vertical transmission. CMV can cause an acute loss of vision
90-100% of the population carries CMV. However, majority are asymptomatic. It is rare to find ocular manifestations of CMV in immunocompetent patients.
| Type of CMV infection | Pt Hx | Signs and Symptoms |
|---|---|---|
| Congenital CMV infection | Baby of mother with acute CMV infection in pregnancy | LBW, microcephaly, petechial rash, seizures, Hepatosplenomegaly, jaundice, cataracts |
| CMV infection | Immunocompromised patient (AIDS, transplant, cancer, dialysis) | Liver failure, CMV colitis, esophagitis, pneumonia, retinitis |
- Signs and symptoms
- Blurry vision
- Floaters
- Retinal detachments
- Investigations
- Treatment
- IV Ganciclovir
- HIV positive patients should be started on HAART
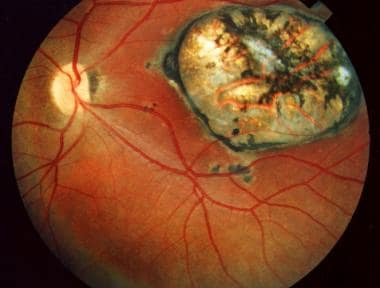
Toxoplasma Retinitis
Toxoplasma gondii causes infection in both immunocompetent and immunocompromised patients. However retinitis typically manifests in immunocompromised patients and in children through vertical transmission. It is transmitted horizontally through exposure to cat litter, undercooked meat and eggs, or unwashed vegetables.
- Signs and symptoms of acute toxoplasmosis Mild flu-like symptoms
- Fever
- Muscle aches
- Lymphadenopathy
- ‘Signs and symptoms in immunocompromised patients
- Encephalitis
- Dermatologic symptoms
- Signs and symptoms of congenital infection
- LBW
- Prematurity
- Jaundice
- Hepatosplenomegaly
- Cataract
- Neurologic deficit
- Ocular signs and symptoms
- Decreased visual acuity
- Floaters
- Investigations
- Fundoscopy
- White fluffy lesion in active retinitis
- Darkened lesions (scar)
- Vitreous haze
- Toxoplasma titres: to determine active infection (IgG vs IgM)
- Fundoscopy
- Treatment
- Pyrimethamine and Sulfadiazine
- Can also be given to immunocompromised patients as prophylaxis
- Corticosteroids (in active infection to reduce inflammation)
- Pregnant women receive Spiramycin to reduce risk of transmission to the fetus
- Pyrimethamine and Sulfadiazine
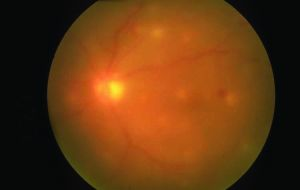
Candida Retinitis
Candida retinitis is the most common fungal infection in the eye. It is typically seen in newborns and other patients with specific risk factors.
- Risk factors
- IV drug use
- Recent major surgery
- Recent sepsis
- Indwelling catheter
- Dialysers
- Cancer patients
- Diabetics
- Newborns of mothers with Candida in the birth canal
- Signs and symptoms
- Decreased visual acuity
- Floaters
- Photophobia
- Pain (candida also affects other structures of the eye)
- Anterior uveitis (red eye)
- Investigations
- Funduscopy
- Dense, white fluffy mass
- Obscured with notable vitreous haze
- Funduscopy
- Treatment
- Amphotericin B and Flucytosine
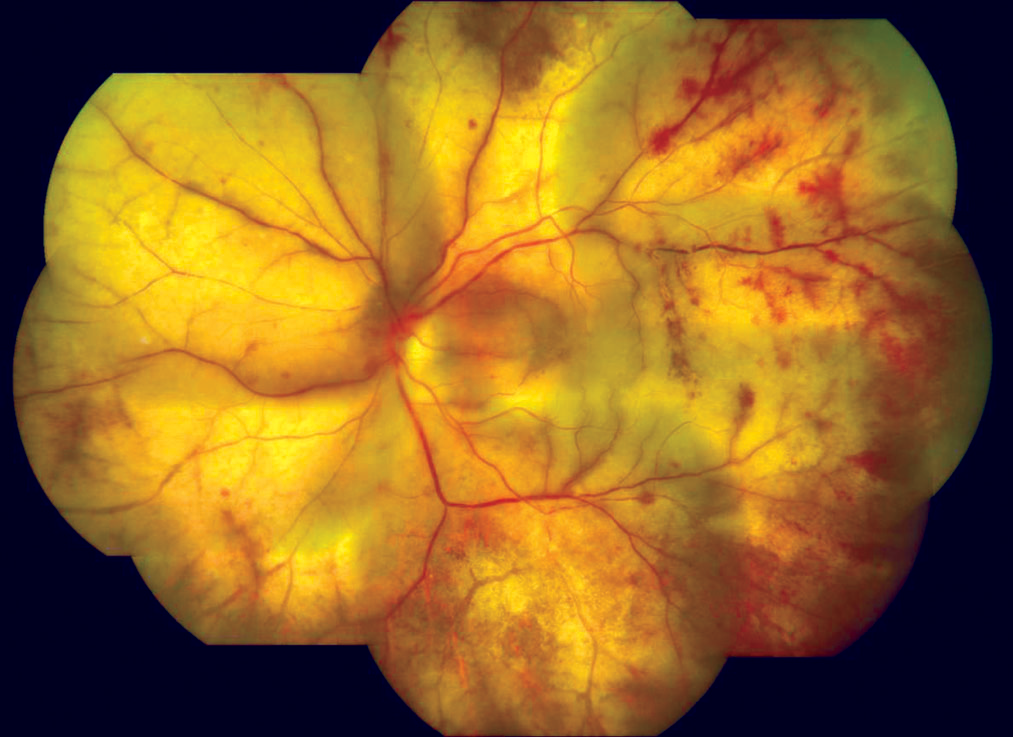
Acute Retinal Necrosis (ARN)
ARN is a sudden infection in young, immunocompetent patients caused by HSV or VZV. It presents with the typical retinitis symptoms. Prognosis is poor.
- Investigations
- Fundoscopy
- Patchy white necrosis
- “Holes” in the peripheral retina progressing towards the posterior pole
- Fundoscopy
- Treatment
- Acyclovir
- Corticosteroids and Aspirin

Progressive Outer Retinal Necrosis (PORN)
PORN is also due to VZV and HSV. It presents similar to ARN but occurs in immunocompromised patients (HIV/AIDS). Prognosis is also poor.
- Investigations
- Fundoscopy
- Homogenous necrosis of the retina
- ”Cracked mud” appearance due to Perivenular sparing (inflammation does not go through the venules and arterioles)
- Cherry red spot
- Fundoscopy
- Treatment
- Ganciclovir + Foscarnet IV
Other Causes of Retinitis
Cryptococcus Retinitis
Syphilis Retinitis
TB Retinitis