Increased heart rate by 10 – 15 bpm, increased stroke volume and cardiac output, increased intravascular volume, decreased systemic vascular resistance, decreased blood pressure in the first and second trimester
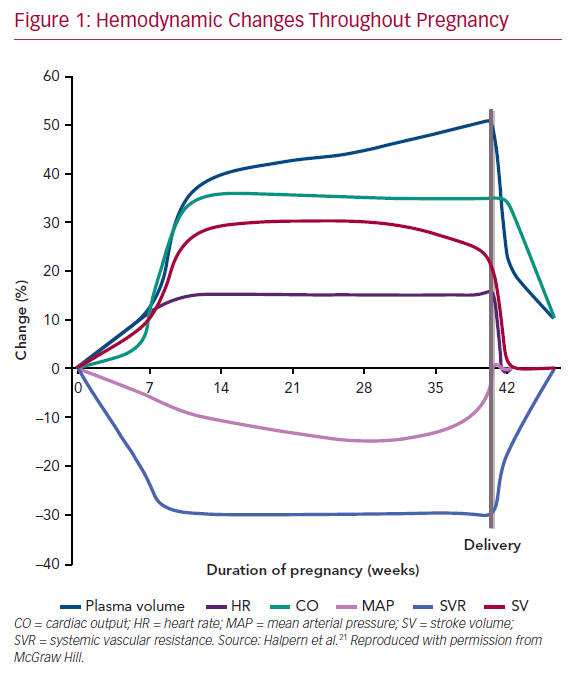
Pregnancy is a high-flow, low-resistance state. Plasma volume increases substantially (2.5 – 3.75 L), especially in multigravidas and women bearing multiple gestations.
How does cardiac output increase during pregnancy?
It increases by 30-50%
Increased stroke volume (30%, predominantly earlier on in pregnancy)
Increased heart rate (15-25%; 10-20bpm, predominantly in the later stages of pregnancy which translates to an average of 80-90bpm)
Why does blood pressure decrease in pregnancy?
Due to a substantial reduction in systemic vascular resistance (20% decrease): shunts blood to kidneys
Diastolic pressure sees the most decrease (10-15mmHg, compared to 5-10mmHg decrease in systolic)
Why does femoral venous pressure (lower venous pressure) increase in pregnancy?
Mechanical factors: the gravid uterus exerts pressure on the IVC, common, and external iliac veins
There is however no change in central venous pressure
Why is there a systolic ejection murmur along the left sternal border?
Normal due to increased flow (diastolic murmurs are pathological and warrant an echo)
Why should women be encouraged to lie on their left side during late pregnancy?
To avoid supine hypotensive syndrome (aortocaval compression syndrome) as cardiac output is highest in the left lateral position (since the uterus no longer compresses the IVC which is located to the right of the midline)
Cardiovascular parameter
Change
Cardiac output
Increases 30-50%
Stroke volume
Increases 30%
Plasma Volume
Increases 50%
Heart rate
Increases 15-25%
Systemic vascular resistance
Decreases 20%
Systolic BP
Slight decrease of 5-10 mmHg
Diastolic BP
Decreases 20% (10-15mmHg)
Central Venous Pressure
No change
Femoral venous pressure
Increases 2-3x
Hemodynamic changes throughout pregnancy
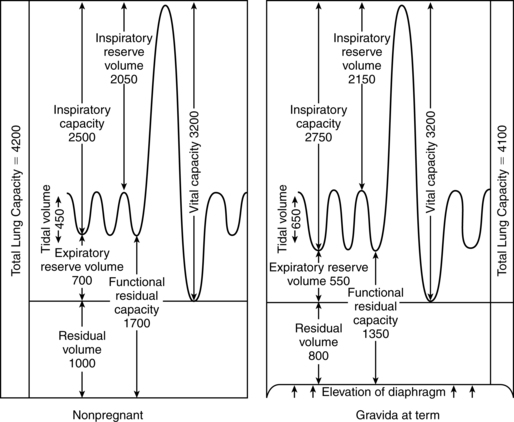
Respiratory Changes
There is increased ventilation in pregnancy which translates into a low arterial CO2 and increased CO2 exchange at the placenta. The respiratory drive increases due to various factors (e.g. progesterone) and leads to a degree of dyspnea.
Why does residual volume decrease by 20% in pregnancy?
The uterus causes elevation (increased excursion) of the diaphragm during exhalation
Why does PaCO2 decrease in pregnancy (chronic respiratory alkalosis)?
Increased ventilation (Ve increases by 40%)
Creates a higher gradient for diffusion from the fetus at the placenta
This state of respiratory alkalosis is compensated by increased HCO3- excretion in the kidneys
What is the action of progesterone at the airway?
Bronchodilation
What is the action of estrogen at the airway?
Edema (Use smaller endotracheal tubes [<6mm] for intubating pregnant women)
Hyperplasia of mucus glands
Consequence of lightening at 36-38 weeks?
The fetal head descends the pelvis, causing less diaphragmatic compression. The woman can breathe easily
However, she is going to have urinary frequency and urgency (the bladder is compressed)
Respiratory prameter
Change
Tidal Volume (Vt)
Increases 30-40%
Minute ventilation (Ve)
Increases 40%
Residual volume
Decreases 20%
PaCO2
Decreases 25%
Oxygen consumption
Increases 20-33%
Pulmonary changes in pregnancy
Hematologic Changes
Hb and HCT go down because of hemodilution (dilutional anemia). Pregnancy is a hypercoagulable state (due to venous stasis and endothelial damage). Iron and folate requirements double during pregnancy. IDA is the most common cause of anemia in pregnancy (Iron study – low ferritin – is diagnostic)
Increased ureteral size, urine glucose, and mechanical factors predispose the patient to pyelonephritis and UTI. There is also some degree of proteinuria. Increased RAAS causes increased total body sodium (however serum concentration remains constant due to dilution.
Effect of lightening
Increased urinary frequency and urgency (but makes it easier to breathe)
Renal parameter
Change
Kidney size
Increases 100%
Ureteral diameter
Increases
GFR
Increases 50%
BUN, Cr, and uric acid
Decreases 25%
Plasma Na
Unchanged
Plasma HCO2
Decreases 20%
Blood pH
Slight increase (7.4 → 7.44)
Urine glucose
Increased
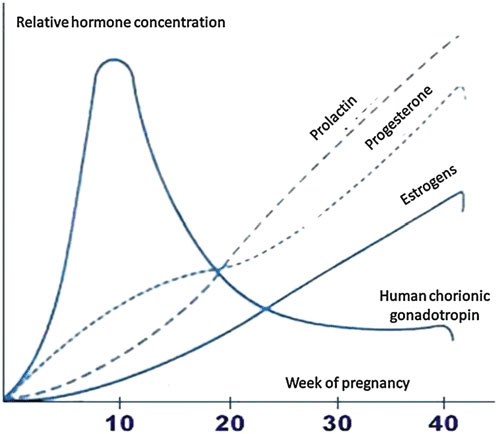
Endocrine Changes
What is the predominant estrogen elevated in pregnancy?
Estriol (produced by the placenta; fetal DHEAS → estriol)
What is the clinical relevance of pituitary hypertrophy?
Renders it vulnerable to ischemia (Sheehan syndrome; post-partum apoplexy following PPH leading to pan-hypopituitarism)
What is the relevance of increased cortisol (increased adrenal activity) in pregnancy?
Favors fetal lung maturity (peaks towards later pregnancy)
Interestingly causes depression; and may render mothers susceptible to post-partum depression
Why does the thyroid increase in size?
Higher levels of hCG which shares an a-subunit with TSH
Mum is however euthyroid (due to increased thyroid-binding globulin)
Human placental Lactogen/Human chorionic somatomammotropin (hPL/hCs)
Most of these are due to mechanical factors (and progesterone). Food sticks around the stomach longer. LES Sphincter tone decreases (among other factors) increasing reflux. More fluid is taken up in the colon causing harder stool (constipation). Increased hCG concentrations are associated with nausea. Hemorrhoids affect 30-40% of women. The stomach is considered “full” at all times during pregnancy ( because the fetus is compressing the stomach, even if NPO for 8-12 hours)
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.