IVH is a commonly encountered in the NICU, particularly in preterm neonates. It is closely associated with Hypoxic Ischemic Encephalopathy. It is the hemorrhage into the germinal matrix capillary bed (tissues surrounding the lateral ventricle). It is typically the result of HIE which disrupts cerebral autoregulation. Antenatal steroids (Dexamethasone) gretly reduces the risk of future development of IVH/PVH. Preterm infants should be screened for IVH/PVH through cranial ultrasound. MRI can be ordered to look at the extent of the damage.
Germinal matrix: immature tissue containing glial cells. It has an immatureVery friable, highly metabolic, and heavily reliable on oxygen.
Factors associated with PVH/IVH and their treatment/prevention
| Contributing factor | Treatment/Prevention |
|---|---|
| Prematurity | Antenatal steroids, Supportive care |
| Birth Asphyxia/HIE | Resuscitation, Supportive care |
| NN seizures | Phenobarbital, EEG monitor |
| Hypertension | Avoid rapid volume expansion |
| Shock | Fluid replacement, monitor U/O |
| Hypercarbia/hypoxia | Adequate oxygenation |
| Metabolic acidosis | Bicarbonate as per neonatologist |
| Anaemia | Blood products as needed |
| Coagulopathy | FFP |
| Rapid volume expansion (iatrogenic) | Avoid |
| Hydrocephalus | Acetazolamide, Surgery |
Classification corresponds to the amount of bleeding
| Grade | Extent of hemorrhage | Prognosis |
|---|---|---|
| Grade I | Hemorrhage of subependymal germinal matrix (PVH) | Good |
| Grade II | Hemorrhage of subependymal germinal matrix extending into the lateral ventricles. No ventricular dilatation (10-15% filled with blood) | Good |
| Grade III | Hemorrhage of subependymal germinal matrix extending into the lateral ventricle with ventricular dilatation | Mortality <10%. 30-40% have cognitive or motor deficits (blindness or Cerebral Palsy) |
| Grade IV | Hemorrhage of subependymal matrix extending into the lateral ventricles with associated ventricular dilation and intraparenchymal hemorrhage | Mortality 80%. 90% will have cognitive or motor deficits. |
- Pathophysiology
- Poorly developed structural support of blood vessels (Immature basal lamina, few pericytes, decreased glial fibers)
- Blood vessels are simple, endothelial-lined and larger than mature capillaries
- These capillaries are prone to hemorrhage
- Impaired autoregulation of cerebral blood flow in premature brain causes inability to maintain constant cerebral blood flow → ishcemia and reperfusion injury
- Long-term complications
- Cerebral palsy
- Periventricular leukomalacia (PVL) – permanent parenchymal damage. Presence of periventricular cysts. Has a tendency to affect lower limb and optic nerve fibers the most.
- Hydrocephalus
- Seizures
- Developmental delay
- Causes of IVH
- HIE
- Asynchrony on mechanical ventilation (give a muscle relaxant to suppress the neonates own respiration)
- Metabolic acidosis
- Hypercarbia or hypoxia
- Vacuum delivery
- Coagulopathy
- Maternal hypertension (elevated BPs in mum → elevated BPs in baby causing bleeding in the germinal matrix)
- Signs and symptoms
- Investigations
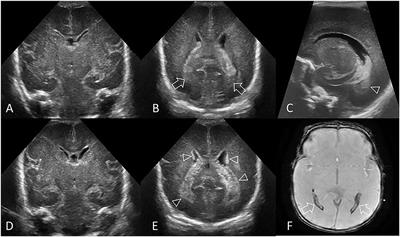
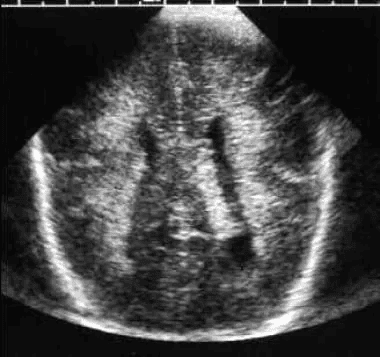
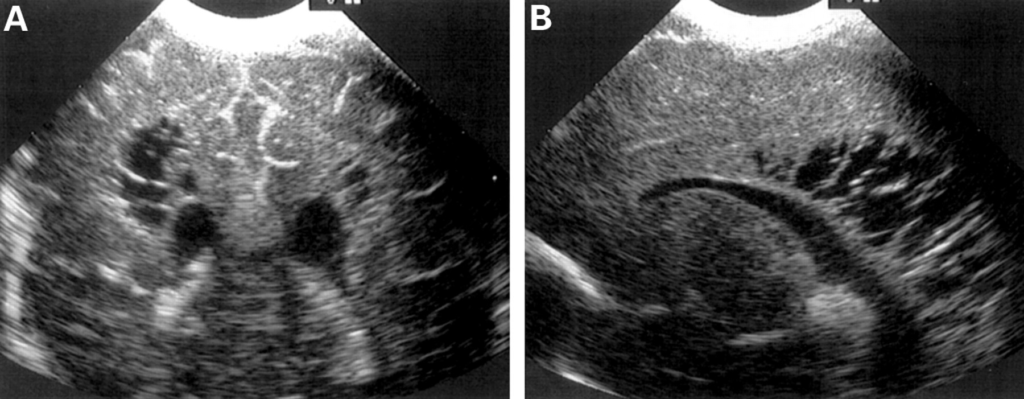
- Cranial ultrasound: best initial test. Can be used to screen neonate infants. Can follow up wth MRI
- Labs
- CBC
- RBC: hypoglycemia
- ABGs: metabolic acidosis
- Coagulation profile
- Treatment
- Admit to NICU
- Umbilical artery catheter placement w/XR confirmation
- Correct metabolic and fluid disturbances
- Refer to neonatologist, paediatric neurosurgeon if hydrocephalus develops – Surgical management
- Long-term follow-up