Firearm Injuries
Firearm injuries occur when someone is shot by a bullet or projectile from a firearm. Injury varies and largely depends on anatomical location and ballistics. The mode of injury depends on the shape, velocity and possible deformation or fragmentation of the missile. Effect of the bullets on bone is dependent on bullet velocity. High-velocity bullets cause bone fragmentation and have the additional effects of cavitation and shock wave injury.
Gunshot wounds can be typical or atypical. The majority seen in practice are atypical, where it may not be clear what is the entry and exit wound.
Definition of terms
| Term | Definition |
|---|---|
| Firearm | An assembly of a barrel and action from which a projectile is propelled through the deflagration (rapid burning) of a propellant (gunpowder) |
| Ammunition | Any material fired, scattered, dropped or detonated from any weapon e.g., gunpowder, bullets, shells, bombs, missiles, grenades, landmines |
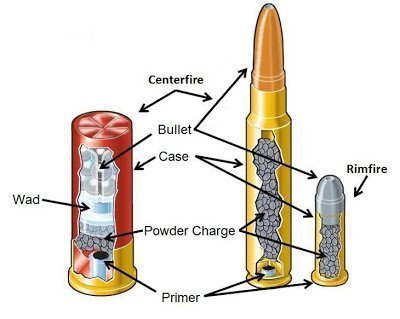
| Cartridge | The unit of ammunition that holds the bullet. It consists of a case, a primer, a propellant (gun-powder), and one or more projectiles. The projectile is the true bullet. |
| Ballistics | The science of motion of projectiles. Includes the study of the effects of discharging and factors affecting the efficacy of firing. |
| Internal ballistics | The study of firearms and projectiles and their motion in the firearm |
| External ballistics | The study of the motion of a projectile after being ejected from the firearm till the target |
| Terminal (wound) ballistics | The study of injuries produced by a firearm |
| Caliber | The caliber of rifled firearms is the distance measured by opposite lands or the inner diameter of the barrel. The caliber of shotguns is equal to the number of pellets of lead which can be made out of 1 pound (450g) of the lead. |
- The examination of firearm wounds allows for the determination of the following aspects of the injuries:
- Range of fire: the muzzle-to-target distance – contact, near contact, intermediate and distant
- Trajectory of the missile or projectile
- Type and extent of the injuries inflicted by the projectile

Firearms
- Mechanism of firing a gun
- Every firearm has a chamber where the catridge is lodged. The chamber leads to a hollow steel tube known as the barrel.
- The spring is released on pulling the trigger
- The proximal end of the chamber has a small hole where a pin move forward to strike the base of the cartridge. The striking action produces heat which ingnites the primer.
- This initiates burning of the powder charge producing extremely hot and explosive gases which propel the bullet or pellets through the barrel and out of the gun
- The bullet is propelled together with a jet of flame, gases, soot from the combustion, and burning and unburnt gun powder (gunshot residues). The detection of these materials on skin in or around the wound is essential to make a diagnosis of contact or intermediate gunshot wound
Classification of firearms
| Classification | Description |
|---|---|
| High velocity firearms (Rifle) | Long-barreled weapon with a stock designed to be braced against the shoulder of the shooter. It also has a rifled barrel (spiralling parallel grooves cut into the barrel to stabilise bullets). |
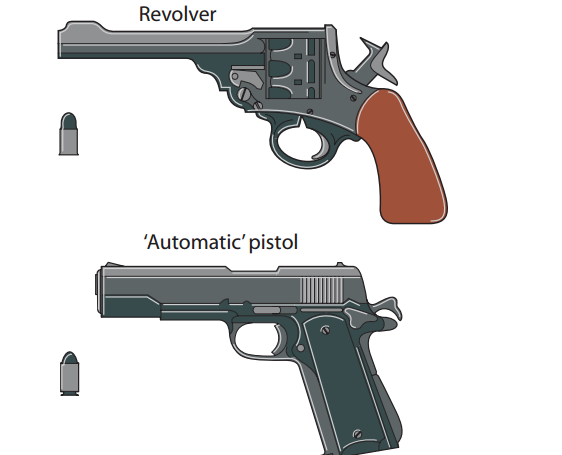
| Low velocity firearms (Handgun) | Rifled. Held by the hands, and are designed to be fired by one or two hands. Does not have any bracing mechanism. Generally has a short barrel relative to other types. Examples: pistols, revolvers |
| Smooth bore firearm (shotgun) | Long barreled weapon with a smooth non-rifled barrel (has no grooves). It usually fires a charge consisting of multiple round shots instead of a single projectile |


Firearm wounds
Definition of terms
| Term | Definition |
|---|---|
| Entry wound | The wound produced by a projectile as it enters the body |
| Exit wound | The wound produced by the projectile as it leaves the body. May be absent sometimes. |
| Track | The path traversed by the projectile between the entry and exit wound |
| Yaw | The angle between the path and the longitudinal axis of the bullet. As the bullet travels through tissue, yaw increases. It may reach upto 90 degrees (creating the widest permanent cavity), and if it continues it travel it eventually makes a complete 180 degree flip and travels backwards. |
- Factors that determine the severity of firearm wound
- Mechanical interaction between the projectile and the tissue
- Effects of the temporary cavity produced by the projectile
- Direct laceration of tissues
- A drilling effect that occurs with any penetrating object. This is the main mechanism in low velocity gunshot wounds.
- Seen in autopsy as a permanent cavity.
- Temporary cavity formation
- This is produced by large amounts of kinetic energy being transferred to the tissue. It is primarily seen in high-velocity gunshot wounds.
- If the pressure of the temporary cavity exceeds the elastic limit of the tissue the organ may be disrupted (”bursting effect”). Inelastic organs such as the liver are susceptible to this.
- Seen in autopsy as a wide zone of hemorrhage that surrounds the small permanent cavity
Firearm Identification
This is done by ballistics, which can be used to identify:
- Type of bullet
- Type of firearm
- Serial number on the weapon
- Gunshot residue pattern on hands clothes or wounds
- Estimation of muzzle-to-target distances
Methods employed include:
- Comparing of rifling marks: as a bullet is expelled through a barrel, the rifling causes it to spin leaving impressions on the bullet surface. These indentations can help to identify the firearm used as no two rifle barrels are alike.
- Cartridge identification: cartridges fired from an automatic firearm show repetitive marks which are useful in the identification of the type of weapon used. Striated action marks imprinted on the cartridge include chamber marks, firing pin drag marks, shear marks and ejector marks.
- Bullet and cartridge comparison: to match bullets to a gun, test bullets must be fired through a suspect firearm for comparison with the crime bullet. This is done using a comparison microscope
- Firearm discharge residue (Gunshot Residue – GSR) identification
- Primer: lead, antimony and barium
- Powder: nitrocellulose, nitroglycerine
- Bullet: Lead, copper, iron
- Cartridge: copper, zinc, nickel
- Barrel: iron, oil
- Greiss test: a test carried out on or around bullet holes to pick up residues of unspent gunpowder. Nitrites are found in incompletely burned powder while nitrocellulose is found in modern smokeless powders. When the Greiss reagent is added to a nitrite-containing sample, it turns pink. The reagent may be sprayed on the hands of a suspect or on the body of the victim, and observed for the colour change
- Sodium rhodizonate test: detects lead residues
- Scanning electron microscopy with an energy dispersive X-ray analyser (SEM-EDX): specific for characteristics and morphological analysis of inorganic gunshot residue particles
Effects of projectiles on the body
- When the missile penetrates the skin it mechanically thrusts aside the tissues along a track wider than the missile
- The tissues are lacerated or crushed. Secondary damage occurs from the rupture of blood vessels and other structures resulting in a permanent wound cavity
- High-velocity projectiles produce cavitation
- Bullets may fragment or bone spicules from fractures may result and act as secondary projectiles to damage tissues
- Pellets from shotguns are spherical balls of lead, that do not travel far, disperse easily and have poorer penetrating ability than bullets. The disadvantage- they are discharged en masse from the barrel and cause extensive damage


Gross examination and findings
- Examine all wounds carefully before cleaning the body, as well as the hands
- Photographs of a wound before and after cleaning should be taken for documentation of the findings
- Compare the wounds noted externally with the number of projectiles found in the body on radiographic examination
- If surgery has been performed, consider that a bullet may have been purposely or inadvertently removed during the procedure
- Localisation and measurement of wounds should be done. Use consistent reference points and anatomical landmarks.
- The wound is generally measured in 2 dimensions and described by its shape
- The presence or absence of any abrasion rim should be noted, as well as any soot or powder stippling. The extent of all these should be measured
Entry wounds
Skin wounds can help to determine the type of wound i.e., whether entry or exit. The skin is elastic and resilient, therefore gunshot perforations may be small and can easily be missed as a result of the initial perforation recoiling to a smaller puncture.
The distance between the muzzle end of the barrel and the target is called the range.
Range
| Range | Distance | Description |
|---|---|---|
| Indeterminate range | Cannot be determined (distant wounds) | Classically a central perforation surrounded by a margin of abraded skin. Typically round to oval with smooth edges. Distant wounds are also classified as determinate |
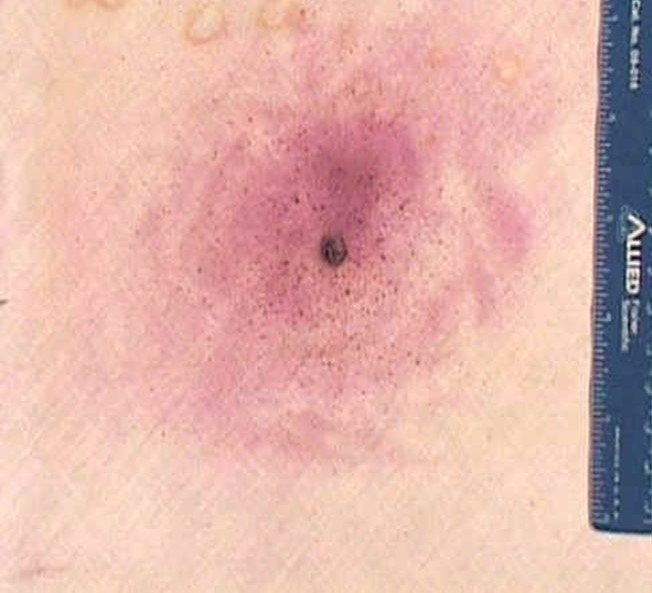
| Intermediate range | 70 cm in handguns and 100 cm in rifles | Defined by the presence of punctate abrasions caused by pieces of gunpowder striking and abrading the skin. These red punctate abrasions are not washed away and are collectively termed stippling (tattooing). Gunpowder deposited on the skin and embedded in the abrasions can be washed away. Clothing and scalp hair may obstruct tattooing and therefore must be closely determined |
| Near contact | 1.5 to 2 cm | Wounds where the gun discharges very close to skin but is not actually in contact with it. The cone of the tattooing is so small and dense that the surrounding skin may appear roughened like sandpaper. This is by peppering of the gunpowder grains while also being blackened by soot and seared by the flame. In angled discharge, the side closer to the muzzle has a wider zone of blackening and searing. |
| Contact range | Contact with skin | Soot and gunpowder residue expelled along with the fired projectile will stain the wound edges dark gray to black. The muzzle of a firearm can leave an ecchymotic or abraded imprint on the skin. Back spatter is present, which refers to the presence of blood and tissue fragments in the muzzle after a close-range discharge. This is due to a suction effect after the pressure of the gas blast subsides, possibly as a result of rapid relative cooling of the skin. It may also soil the hand or arm of the person firing the gun, which would be significant evidence |
| Hard contact | Pressed firmly onto skin | Results in tears that impart a stellate configuration to the wound. Frequently seen in gunshot wounds to the head, where the hot expanding gases forced between the scalp and calvarium are released by creating tears in the scalp |





Shotgun wounds
- A contact shotgun wound will resemble that of a single projectile, as the shot charge enters the body en masse
- As the muzzle-to-target distance increases, a more irregular entrance wound with scalloped edges may occur due to early pellet spread
- As the distance becomes a few metres, the margin of the wound will become rugged
- At a slightly longer distance, individual satellite defects may be seen around the main wound due to individual pellet strikes
Exit wounds
They are more irregular than entrance wounds. They are NOT associated with muzzle imprinting, searing, soot deposition or stippling. The edges are often torn, resulting in a stellate configuration or a rugged appearance. There may not be a central defect once the skin edges are approximated. They have no abrasion rim.
In the event of a low-velocity exit, they have a slit-like configuration which is deceptively sharp-appearing and can mimic a stab wound. Exit wounds are not always larger than entry wounds, and a protrusion of fat and viscera is not always a feature of all exit wounds (herniation may occur due to gravity or pressure).

- Differences between a typical entry and exit wound Entry wound Exit wound Margins Regular outline with a punched out appearance Irregular, jagged, erratic and lacerated Rim of abrasiion Usually has a rim of abrasion Usually no rim of abrasion unless the body was pressed against a surface Size Smaller, although in high velocity injuries it may be larger than the exit wound Larger Edges Inversion of the edges of the wound Eversion of the edges of the wound
Atypical wounds
Occur due to the instability of the bullet as it loses speed or passes through a first target first, or is obstructed by a door or a window. The wounds are usually irregular. Obstructions may also cause bullets to fragment, leading to the creation of secondary missiles which cause multiple punctate wounds referred to as ‘pseudo-tattooing’.
Microscopic examination and findings
Wounds may show crush of tissue with haemorrhage on histological examination. If the interval between injury and death is long, typical healing changes may be present. Soot and gunpowder grains may also be seen particularly in the case of contact wounds, which will also show superficial thermal alteration of the tissues.
Self-inflicted (suicidal) firearm wounds
- Suicide notes are found in a minority of such cases
- The weapon must always be present
- The range must be within arm’s length, depending on the nature of the weapon and excluding some mechanical device to fire the gun
- Sites of election include the temple, neck, mouth, and chest. Rarely do the patients shoot themselves in the eye or abdomen
- Suicidal wounds will either be contact or intermediate range
- Multiple firearm wound suicides are not common
| Suicidal | Homicidal | |
|---|---|---|
| Site of entry wound | Head or chest | Any part |
| Range | Contact or close | Any range |
| Number of wounds | Usually One | One or multiple |
| Firearm residue on hand or blood spatters on hand | Present | Usually absent |
| Weapon at the scene | Usually present | Usually absent |
| Suicide note | Usually present | Usually absent |
| Motive | Depression | Robbery, revenge, rape, sexual-related attack e.t.c. |
| Other injuries on the body | Usually absent | Usually present |
