Cardiovascular
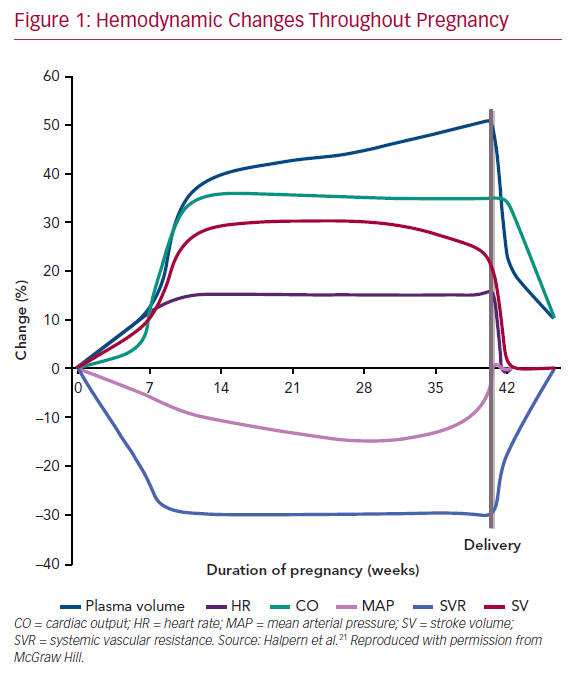
Pregnancy is a high-flow, low-resistance state. Plasma volume increases substantially (2.5 – 3.75 L), especially in multigravidas and women bearing multiple gestations.
- How does cardiac output increase during pregnancy?
- It increases by 30-50%
- Increased stroke volume (30%, predominantly earlier on in pregnancy)
- Increased heart rate (15-25%; 10-20bpm, predominantly in the later stages of pregnancy which translates to an average of 80-90bpm)
- Why does blood pressure decrease in pregnancy?
- Due to a substantial reduction in systemic vascular resistance (20% decrease): shunts blood to kidneys, thy
- Diastolic pressure sees the most decrease (10-15mmhg, compared to 5-10mmHg decrease n systolic)
- Why does Femoral venous pressure (lower venous pressure) increase in pregnancy?
- Mechanical factors
- The gravid uterus exerts pressure on the IVC, common, and external iliac veins
- There is however no change in central venous pressure
- Mechanical factors
- Why is there a systolic ejection murmur along the Left sternal border
- Normal due to increased flow (diastolic murmurs are pathological and warrant an echo)
- Why should women be encouraged to lie on their left side during late pregnancy?
- To avoid supine hypotensive syndrome (aortocaval compression syndrome) as cardiac output is highest in the left lateral position (since the uterus no longer compresses the IVC)
| Cardiac output | Increases 30-50% |
|---|---|
| Stroke volume | Increases 30% |
| Plasma Volume | Increases 50% |
| Heart rate | Increases 15-25% |
| Systemic vascular resistance | Decreases 20% |
| Systolic BP | Slight decrease of 5-10 mmHg |
| Diastolic BP | Decreases 20% (10-15mmHg) |
| Central Venous Pressure | No change |
| Femoral venous pressure | Increases 2-3x |
Pulmonary
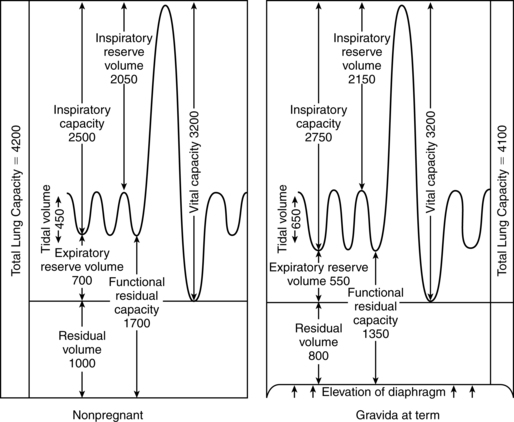
There is increased ventilation in pregnancy which translates into a low arterial CO2 and increased CO2 exchange at the placenta. The respiratory drive increases due to various factors (e.g. progesterone) and leads to a degree of dyspnea.
- Why does residual volume decrease by 20% in pregnancy?
- The uterus causes elevation (increased excursion) of the diaphragm during exhalation
- Why does PaCO2 decrease in pregnancy?
- Increased ventilation (Ve increases by 40%)
- Creates a higher gradient for diffusion from the fetus at the placenta
- This state of respiratory alkalosis is compensated by increased HCO3- excretion in the kidneys
- What is the action of progesterone at the airway?
- Bronchodilation
- What is the action of Oestrogen at the airway?
- Edema (Use smaller endotracheal tubes (<6mm) for intubating pregnant women)
- Hyperplasia of mucus gland
- Consequence of lightening at 36-38 weeks?
- The fetal head descends the pelvis, causing less diaphragmatic compression. The woman can breathe easily
- However, she is going to have urinary frequency and urgency (the bladder is compressed)
| Tidal Volume (Vt) | Increases 30-40% |
|---|---|
| Minute ventilation (Ve) | Increases 40% |
| Residual volume | Decreases 20% |
| PaCO2 | Decreases 25% |
| Oxygen consumption | Increases 20-33% |
Hematologic
Hb and HCT go down because of hemodilution (dilutional anemia). Pregnancy is a hypercoagulable state (due to venous stasis and endothelial damage). Iron and folate requirements double during pregnancy. IDA is the most common cause of anemia in pregnancy (Iron study – low ferritin – is diagnostic)
- Consequence of hypercoagulability in pregnancy
- 5x increases risk of DVT
- Women with inherited hypercoagulability are predisposed to placental vascular thrombosis increasing the risk of:
- Pre-eclampsia
- Gestational hypertension
- Fetal complications (Miscarriage, SGA, Stillbirth)
| Plasma volume | Increases 50% |
|---|---|
| RBC volume | Increases 20-30% |
| Hematocrit | Decreases |
| WBC count | Increases slightly |
| ESR | Increase |
| Coagulation factors | Increase |
| Coagulability | Increase |
| Platelet count | Unchanged |
Renal
Increased ureteral size, urine glucose, and mechanical factors predispose the patient to pyelonephritis and UTI. There is also some degree of proteinuria. Increased RAAS causes increased total body sodium (however serum concentration remains constant due to dilution.
- Effect of lightening
- Increased urinary frequency and urgency (but makes it easier to breathe)
| Kidney size | Increases 100% |
|---|---|
| Ureteral diameter | Increases |
| GFR | Increases 50% |
| BUN, Cr, and uric acid | Decreases 25% |
| Plasma Na | Unchanged |
| Plasma HCO2 | Decreases 20% |
| Blood pH | Slight increase (7.4 → 7.44) |
| Urine glucose | Increased |
Endocrine
- What is the predominant estrogen elevated in pregnancy?
- Estriol (produced by the placenta; fetal DHEAS → estriol)
- What is the clinical relevance of pituitary hypertrophy?
- Renders it vulnerable to ischemia (Sheehan syndrome; post-partum apoplexy following PPH leading to pan-hypopituitarism)
- What is the relevance of increased cortisol (increased adrenal activity) in pregnancy?
- Favors fetal lung maturity (peaks towards later pregnancy)
- Interestingly causes depression; and may render mothers susceptible to post-partum depression
- Why does the thyroid increase in size?
- Higher levels of hCG which shares an a-subunit with TSH
- Mum is however euthyroid (due to increased thyroid-binding globulin)
- Human placental Lactogen/Human chorionic somatomammotropin (hPL/hCs)
- Increases lipolysisAntagonizes insulin to increase blood glucose (pseudo insulin resistant state)
| Estrogen | Increases |
|---|---|
| Progesterone | Increases |
| Pituitary size | Increases 100% |
| Adrenal size | Unchanged |
| Thyroid size | Increases 10-15% |
| Total thyroid hormone | Increases |
| Thyroid binding globulin | Increases |
| Free thyroid hormone | Unchanged |
| Human placental lactogen | Increases |

Hormonal changes during pregnancy
Gastrointestinal
Most of these are due to mechanical factors (and progesterone). Food sticks around the stomach longer. LES Sphincter tone decreases (among other factors) increasing reflux. More fluid is taken up in the colon causing harder stool (constipation). Increased hCG concentrations are associated with nausea. Hemorrhoids affect 30-40% of women. The stomach is considered “full” at all times during pregnancy ( because the fetus is compressing the stomach, even if NPO for 8-12 hours)
- What contributes to reflux in pregnancy?
- Relaxed gastroesophageal sphincter
- Increased emptying time
- Decreased gastric motility
- Increased gastric pressure (mechanical)
- Management of reflux in pregnancy
- Avoid trigger foods (chocolate, caffeine, alcohol)
- Treat with H2 blocker (cimetidine, ranitidine); try avoiding PPIs; can also use metoclopramide (anti-emetic that increases gastric motility)
- Hyperemesis gravidarum
- Severe nausea during pregnancy that is associated with a decrease in pre-pregnancy body weight of at least 5%.
- Described as a really bad morning sickness…
- Treatment: frequent snacking and antiemetics (doxylamine/B6)
| Gastric motility | Decreases |
|---|---|
| Gastric emptying time | Increases |
| GES tone | Decreases |
| Colonic motility | Decreases |
| Colonic transit time | Increase |
Dermatologic
- Striae gravidarum
- Stretch marks along the abdomen and buttocks
- More cortisol
- Belly stretches
- Genetic predisposition
- Stretch marks along the abdomen and buttocks
- Linea nigra and increased pigmentation of the areola
- Increased pigmentation of the abdominal midline at 22-24 weeks/beginning of 3rd trimester
- Due to increased MSH
- May witness occasional light linea nigra on baby during birth (MSH can cross placenta)
- Increased pigmentation of the abdominal midline at 22-24 weeks/beginning of 3rd trimester
- Chloasma/Melasma
- Blotch pigmentation of the nose and face – “Mask of pregnancy”
- Increased MSH
- Increased vascularity
- Blotch pigmentation of the nose and face – “Mask of pregnancy”
- Spider angiomata and palmar erythema
- Stigmata resulting from increased vascularity
- Chadwick sign
- Bluish/purplish discoloration of the vagina and cervix
- due to increased vascularity
- Bluish/purplish discoloration of the vagina and cervix

Linea nigra with striae gravidarum

Chloasma