Fibroids are benign smooth muscle neoplasms arising from myometrial cells. Usually clinically insignificant but VERY common (it is the most common benign tumour in women). Average growth is 0.5 cm/yr. Fibroids are estrogen and progesterone-sensitive (similar to endometriosis and adenomyosis).
The most common type of fibroid is intramural. Submucosal and intramural fibroids are the most problematic for fertility (can lead to abnormal implantation). Most fibroids are asymptomatic. They are detected on physical exam as uterine enlargement with irregular contour. Most fibroids are minimally asymptomatic and can be managed by patient education and annual surveillance.
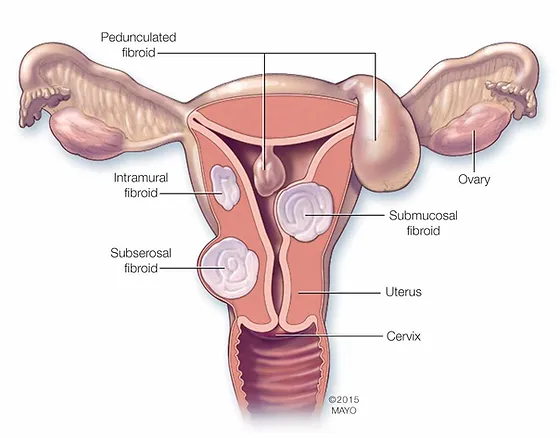
Uterine fibroids
- How do Leiomyomas create a hyperestrogenic environment?
- Contain more estrogen receptors
- Convert less estradiol to estrone
- Contain more aromatase
- What is the effect of progestins on leiomyomas?Unclear
- Given alone, progestins decrease growth
- Given with GnRH agonists, progestins accelerate growth
- Risk factors for fibroids
- Incidence increases with age during reproductive years (30-40 yo)
- African origin
- Family history (2X risk with primary relative)
- Overweight/obesity
- Early menarche
- PCOS
- Risk-reducing factors
- Risk decreases with parity
- Giving birth at an ealry age
- COCs
- Smoking?
- Signs and symptoms
- Abnormal bleeding (usually menorrhagia; most common sx)
- Dysmenorrhea
- Dyspareunia
- Noncyclical pelvic pain
- Infertility (2-3% cases of infertility)
- Acute pelvic pain (d/t degeneration or torsion of pedunculated leiomyomas)
- Physical examination
- Uterine enlargement with irregular contour
- Non-tender or minimally tender
- Uterine enlargement with irregular contour
- Types of degeneration2/3 of fibroids undergo degeneration
- Hyaline degeneration(most common, clinically insignificant – connective tissue replaces smooth muscles as fibroids lose their blood supply)
- Red degeneration (Carneous degeneration – common during or after pregnancy as an enlarged uterus compresses venous outflow from the fibroid causing hemorrhagic necrosis)
- Cystic degeneration (post-menopause as necrosis happens – can look like a mole in women of childbearing age.)
- Liquefactive
- Muocid
- Fatty
- Calcification
- Sarcomatous (malignant)
- Investigations
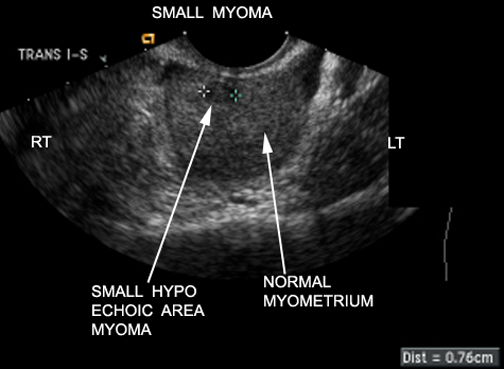
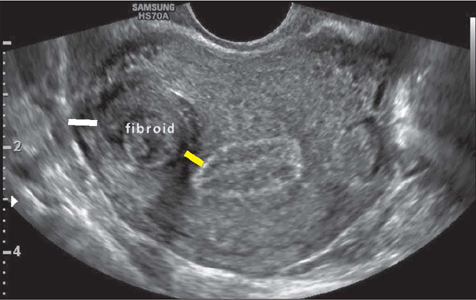
- Transvaginal ultrasound: imaging modality of choice. Saline infusion can be performed to delineate the anatomy of the uterus (for intracavitary fibroids)
- Hyperechoir or hypoechoic discrete masses
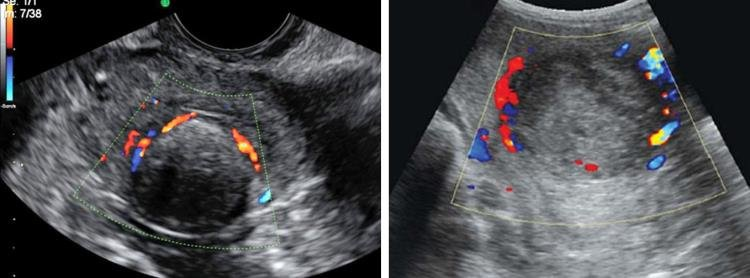
- Doppler shows a rim of blood flow around the fibroid
- Other labs
- Urine B-hCG
- CBC
- Transvaginal ultrasound: imaging modality of choice. Saline infusion can be performed to delineate the anatomy of the uterus (for intracavitary fibroids)
- Medical Treatment
- NSAIDs: for pain and dysmenorrhea
- Combined Oral Contraceptives: for pain and menorrhagia
- LNG-IUS (Mirena): for pain, menorrhagia (***sufficient distortion of the uterus can dislodge the intrauterine device)
- GnRH agonists (Leuprolide, Nafarelin, Goserelin, Buserelin): effective for fibroids refractory to COCs. Have a variety of side effects related to low estrogen. ACOG recommends not to use these for more than 6 months without add-back therapy.
- Surgical Treatment
- Uterine artery embolization (can get post-embolization syndrome – very painful)
- Myomectomy: laparoscopic, hysteroscopic, or open. Preferred if fertility is the main issue of concern (however, will need elective C-sections to deliver)
- Hysterectomy
- Obstetric complications of fibroids
- Miscarriage
- Preterm delivery
- Fetal malpresentation
- Fetal growth restriction
- Abnormal placentation

- Gross appearance
- Elliptical
- Pearly white
- Firm
- Rubberyc consistency
- Covered by a distinct connective tissue capsule
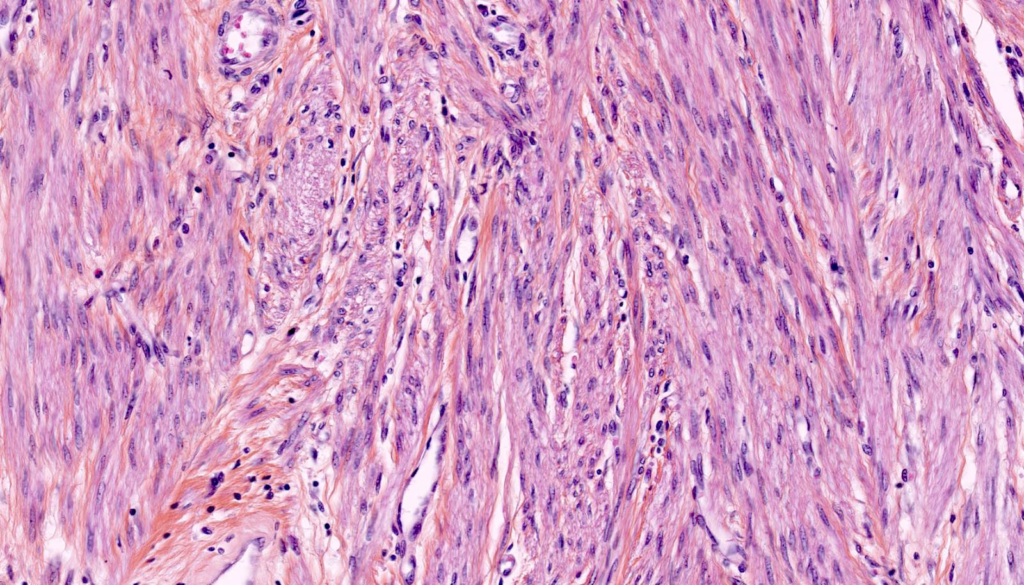
- Histology
- Elongated smooth muscle cells aggregated in bundles
- Minimal to no mitotic activity
- Lack of vascular organization