Acute Appendicitis
Appendicitis is inflammation of the vermiform appendix. It is commonly caused by obstruction of the appendiceal lumen by a fecalith. Appendicitis is one of the most common surgical emergencies and should be on your differential in any patient presenting with acute abdominal pain, especially in the right lower quadrant.
The incidence peaks in teens and young adults (10 – 19 years old). There is a slight male preponderance, but it is common in all groups. Incidence is increasing due to low dietary fiber intake.
- Causes
- Lymphoid hyperplasia (MCC in children and young adults; can be physiological or secondary to an inflammatory process in the bowel)
- Obstruction by fecalith (MCC in adults)
- Neoplasm (likely in older pts)
- Infestation (Enterobius vermicularis, Ascaris lumbricoides, Taenia sp. Schistosoma sp.)
- Pathophysiology of obstructive acute appendicitis
- The appendix is a blind loop (its distal end is closed)
- Obstruction of the proximal lumen creates a closed-loop obstruction
- Mucus is secreted and accumulates within the closed-loop causing pressure to build up in the appendix
- The appendix distends and intraluminal pressure exceeds venous pressure leading to venous congestion. Pressure continues to increase until arterial inflow is compromised
- The areas with the poorest blood supply become ischemic and gangrenous. This allows bacteria to translocate into the mucosa and submucosa
- The wall becomes weakened and perforate (usually at the antimesenteric border just beyond the point of obstruction where tension is high)
- Signs and symptoms
- Anorexia
- “Hamburger sign”
- Unlikely to be appendicitis if there is no loss of appetite
- This is usually the first symptom to appear
- Migratory abdominal pain
- “Pointing sign”
- From umbilicus to the right lower quadrant
- Nausea and Vomiting
- Low-grade fever
- Anorexia
- Signs of localized peritonitis in the RLQ
- McBurney’s sign
- Maximum tenderness at McBurney’s Point
- Blumberg’s sign in the RLQ
- RLQ Rebound Tenderness
- Iliopsoas sign
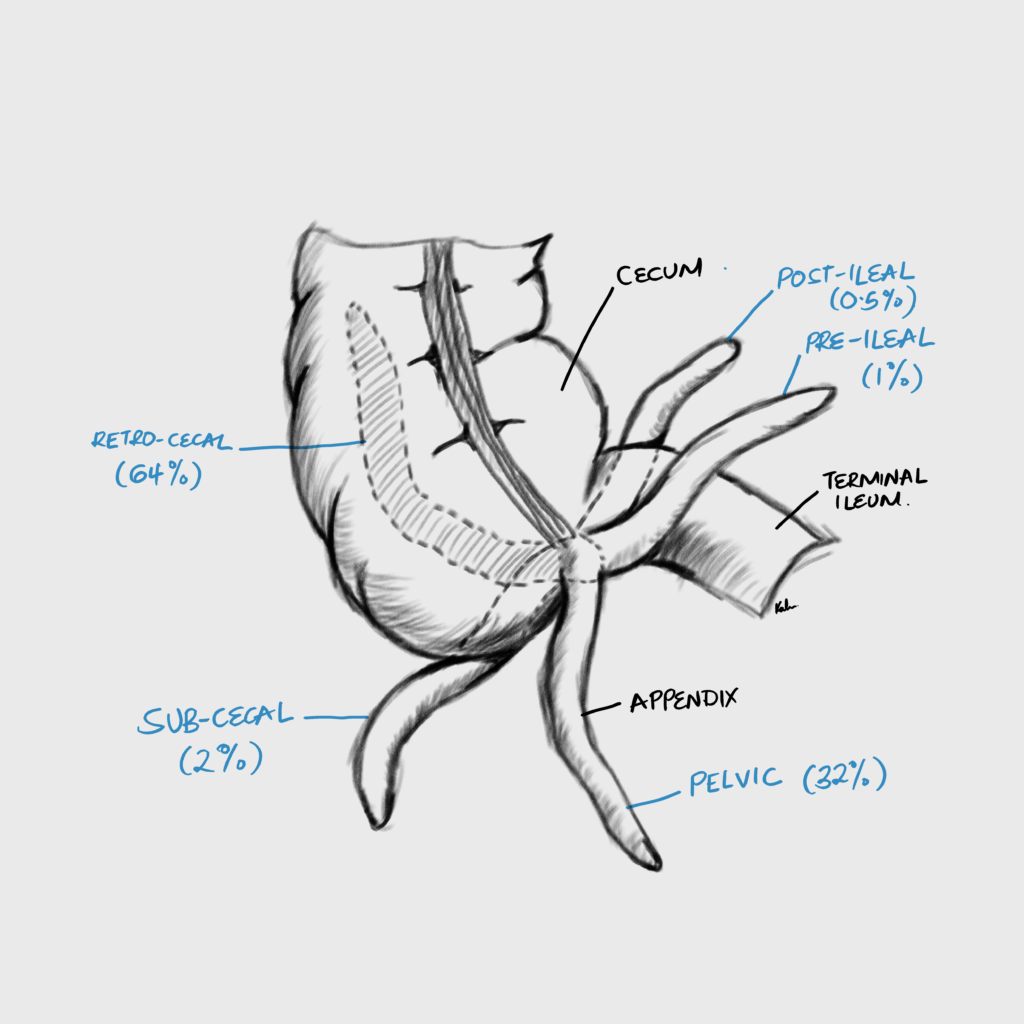
- RLQ pain on active hip flexion (Retrocecal appendix – sits on psoas)
- Baldwing sign
- Flank pain when flexing the right hip (retrocecal appendix)
- Obturator sign
- RLQ pain on abduction of the right hip (Pelvic appendix – sits on obturator internus)
- Rovsing’s sign
- RLQ tenderness elicited on deep palpation of the LLQ
- Due to stretching of the abdominal wall which irritates the peritoneum in the RLQ
- Can also be due to increased pressure on the descending colon which transmitted to cecum and appendix
- Hyperasthesia in Sherren’s triangle
- “Pinch and inch”
- Sherren’s triangle is formed by the ASIS, umbilicus and symphysis pubis
- Lanz point tenderness
- Tenderness at the junction of the right third and left 2/3 of a line connecting both ASIS
- Pain in the pouch of Douglas
- Elicited on DRE
- Dunphy sign
- Sharp RLQ pain elicited by voluntary cough
- Markle sign
- RLQ jar tenderness
- McBurney’s sign
- Differentials for RLQ abdominal pain
- Appendicitis: Anorexia, periumbilical pain → right lower quadrant pain, vomiting, Psoas sign, Rovsing sign
- Perforated peptic ulcer: sudden onset abdominal pain that started in the epigastrium passing down the paracolic gutter, referred to the shoulder, H/O chronic dyspepsia
- Ureteric colic due to urolithiasis: severe intermittent colicky flank pain radiating to the groin without fever
- Diverticulitis: elderly patient with H/O westernised diet, irregular bowel habits, constipation
- Typhoid: fever, diarrhoea, and diffuse abdominal pain
- Amoebiasis: H/O blood-stained mucoid diarrhoea
- Regional enteritis: H/O abdominal cramping, weight loss and diarrhoea
- Right sided pyelonephritis: Increased frequency of micturition, loin tenderness, pyuria and fever (39 degrees celsius)
- Testicular torsion: Testicular pain, swollen and tender testis, lost cremasteric reflex
- Acute pancreatitis: Severe epigastric pain with nausea, vomiting and anorexia. Best ruled out by checking the serum amylase levels.
- Rectus sheath hematoma: Localised pain with no gastrointestinal symptoms with a H/O of strenuous physical activity or mild trauma.
- Carcinoma of the caecum: Especially in the older population. Altered bowel habits, unexplained anaemia and a palpable mass are characteristic
- Hernia incarceration: H/O abdominal pain, constipation, vomiting
- Inflammatory bowel disease: H/O abnormal bowel habits
- Differentials for RLQ abdominal pain in women
- Right-sided ectopic pregnancy: Amenorrhoea (about 6-8 weeks LNMP), right-sided abdominal pain, vaginal bleeding, cervical motion tenderness, adnexal mass, breast tenderness, anaemia, positive pregnancy test (rarely hemorrhagic shock)
- Ovarian torsion: Acute onset severe pelvic/ lower abdominal pain, adnexal mass, H/O ovarian cyst
- Pelvic inflammatory disease: pelvic/lower abdominal pain, purulent vaginal discharge, cervical motion tenderness, adnexal tenderness, dysuria, dysmenorrhea, Neisseria gonorrhea and Chlamydia are the usual suspects.
- Tubo-ovarian abscess: tender fixed fluctuant mass on the right side. H/O of pelvic peritonitis suggests that the abscess may have ruptured
- Mittelschmerz: mild unilateral lower abdominal pain that occurs midcycle, duration from few hours to few days, normal pelvic exam, no fever, negative pregnancy test
- Differentials for RLQ abdominal pain in children
- Mesenteric lymphadenitis: current or recent URTI (nasal discharge, cough, throat pain, etc.), high fever, generalized abdominal pain, tender lymphadenopathy in small bowel mesentery, cervical lymph nodes are enlarged.
- Yersinia enterocolita (pseudoappendicitis): RLQ pain, vomiting, bloody diarrhoea, H/O sick contacts e.g. infected children at daycare
- Pneumococcal pneumonia: Pneumonia associated with nausea and vomiting, and diffuse abdominal pain. Findings on chest auscultation and chest x ray will confirm diagnosis.
- Gastroenteritis: Nausea, vomiting, watery diarrhoea (viral) or bloody diarrhoea (bacterial), myalgia, fever, H/O of contact with contaminated food and people with similar symptoms.
- Intussusception: Nausea, vomiting, crampy abdominal pain, “red currant jelly” stool, “sausage-shaped mass” in the abdomen
- Meckel’s diverticulum: Painless rectal bleeding (current jelly stool). Abdominal pain may be left or centrally placed
- Henoch Schonlein purpura: Preceded by a URTI. Characterised by rashes on the extensor surfaces of the limbs and buttocks, joint pain as well as renal manifestations such as microscopic hematuria.
- Investigations
- Labs
- CBC: elevated WBC, Left-shift
- Comprehensive Metabolic Panel (U/E/C, RBS, LFTs): unremarkable
- Urinalysis: r/o urolithiasis and cystitis
- b-hCG (of upmost importance in women of child-bearing age 12/13 – 55y of age): usually unremarkable but pregnant women can get appendicitis too!
- Imaging
- RLQ ultrasound: best initial imaging tests, esp. for women and children
- Distended appendix > 6mm
- Target sign (appendiceal lumen and edematous muscularis = hypoeachoic, inflammed mucosa hyperechoic)
- Fecalith (focal hyperechogenicity w/posterior acoustic shadowing)
- Noncompressible, aperistaltic, distended appendix (perforated appendix is compressible)
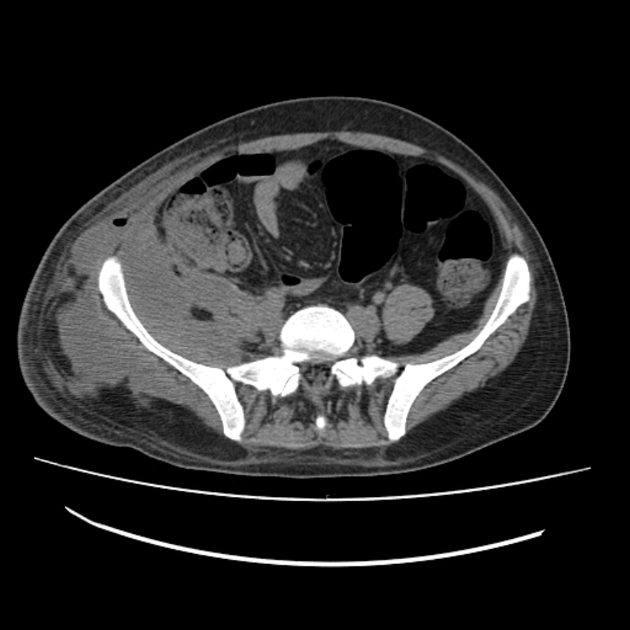
- Abdominal CT with Contrast: Best initial diagnostic test if dx of acute appendicitis is questionable based on hx, px, and labs. 100% accuracy. No contrast in appendix.
- Distended appendix > 6mm
- Edematous appendix w/periappendiceal fat stranding
- Fecalith (focal hyperdensity within lumen)
- Halo or target sign
- RLQ ultrasound: best initial imaging tests, esp. for women and children
- Labs
- Treatment
- Admit
- Oxygen if needed
- Pain meds
- IV Antibiotics (Cover Gram negative and Anerobes that may spill out into peritoneum)
- Do not extend past 24h post op in uncomplicated appendicitis
- Given for 3-5 days post op if complicated
- IV fluids
- Nil per oral
- Surgery
- Appendectomy within 24 hours
- Emergency appendectomy within 8 hours (if there is sepsis or generalized peritonitis)
- Interval appendectomy 6-8 weeks following resolution of acute episode (to minimize surgical compications)
- Relative contraindications to appendectomy within 24 hours
- Appendiceal mass
Both appendiceal mass and abscess are associateed with immediate complications (hemororrage, ileocecal resection, injury to adjacent organs), and late complications (SSI, fistula formation) . They can be treated conservatively and interval appendectomy performed later



Alvarado’s Score (MANTRELS)
Appendicitis is majorly a clinical diagnosis. A 10 point scoring system using clinical criteria to estimate the likelihood of appendicitis. Uses 3 symptoms, 3 physical exam findings and 2 laboratory parameters.
≤ 4 = Low likelihood
5 – 6: Moderate likelihood
≥ 7: High likelihood
| Parameter | Score |
|---|---|
| Migration of pain to RLQ | 1 |
| Anorexia | 1 |
| Nausea and/or vomiting | 1 |
| Tenderness in RLQ | 2 |
| Rebound pain | 1 |
| Elevated temperature > 37.3 C | 1 |
| Leukocytosis > 10,000/mm3 | 2 |
| Shift to the left ≥ 75% Granulocytes | 1 |
Missing the diagnosis of appendicitis
A diagnosis of appendicitis can be missed in patients who present with acute abdominal pain. The pain pain may have started some time/days ago, especially when the patient sought care within the last few days and was discharged without the diagnosis of acute appendicitis i.e. a diagnosis of gastroenteritis was made instead. The abdominal pain has persisted for a longer period of time. By this point the appendix may have ruptured and symptoms may go from RLQ pain to diffuse abdominal pain.
- Patient History
- Recent symptoms consistent with acute appendicitis (RLQ pain, N/V, Anorexia, Fever)
- Symptoms
- Ongoing abdominal pain
- RLQ
- Diffuse (suggest perforation)
- Nausea and vomiting
- Fever
- May be absent due to OTC antipyretics
- Ongoing abdominal pain
- Physical exam
- Generalized guarding/ rebound tenderness (suggest rupture)
- Tenderness at McBurnery’s pint
- Psoas sign
- Obturator sign
- Investigation
- Abdominal CT: Best initial test
- Shows perforated appendix
- Possible abscess
- Abdominal CT: Best initial test
- Treatment
- Admit
- NPO
- Broad spectrum IV antibiotics
- Observe with serial vitals, physical exam, CT scan, and labs (monitor fever, size of the mass, white cell count and pain)
- CT guided percutaneous drainage or Surgical drainage of the abscess
- Discharge when pain and fever subside
- Return for interval appendectomy in 6 – 8 weeks
Complicated Appendicitis
- Complicated appendicitis
- Perforated appendix
- Gangrenous appendicitis
- Appendiceal abcess
- Appendiceal phlegmon
- Pyelephlebitis
- Complications of appendectomy
- Adhesions
- General Surgical complications
- Abscess (SSI)
- Urinary retention etc.
Perforated appendix
A perforated appendix is rupture of the appendix producing signs and symptoms of peritonitis and subsequent abscess formation
- Signs and symptoms
- Generalized peritonitis
- Rigidity
- Guarding
- Rebound tenderness
- Percussion tenderness
- Decreased bowel sound
- RLQ mass (abscess)
- Generalized peritonitis
- Treatment
- Pain meds
- IV antibiotics
- IV fluids
- NPO
- Emergency appendectomy
- If abscess Interval appendicitis after drainage
Gangrenous appendix
Gangrenous appendicits is gangrenous necrosis of the appendiceal wall. It is usually diagnosed intra-op (appendix appears mottled and purple)
- Signs and symptoms
- Severe RLQ pain
- High-grade fever
- Tachycardia
- Treatment
- IV fluids
- Pain meds
- Analgesia
- IV antibiotics
- Nil per oral
- Emergent appendectomy
Appendiceal abcess
An appendiceal abscess is a localized collection of pus around an inflammed appendix, typically after perforation.
- Signs and symptoms
- Tender RLQ mass
- High-grade fever
- Decreased bowel sounds (paralytic ileus)
- Sepsis (Tachycardia, high-grade fever, AMS etc.)
- Treatment
- Conservative
- NPO
- Pain meds
- IV fluids
- Analgesia
- Abscess > 4 cm: surgical drainage
- Consider interval appendectomy
- Conservative
Appendiceal phlegmon
An appendiceal phlegmon is an ill-defined mass of inflammed periappendiceal tissue
- Signs and symptoms
- Tender RLQ mass
- Treatment
- Conservative
- Pain meds
- IV antibiotics
- IV fluids
- NPO
- Interval appendectomy
- Conservative
Portal Pyelophlebitis
Portal pyelephlebitis is septic thrombosis of the branches of the portal vein typically as a complication of perforated appendicitis (intra-abdominal sepsis). Thrombosis of the portal vin can lead to bowel infarction and death.
- Signs and symptoms
- Fever
- Abdominal pain
- Investigations
- CT abdomen
- Filling defect in the portal vein or its branches
- CT abdomen
- Treatment
- IV antibiotics