Last updated:
March 8, 2026
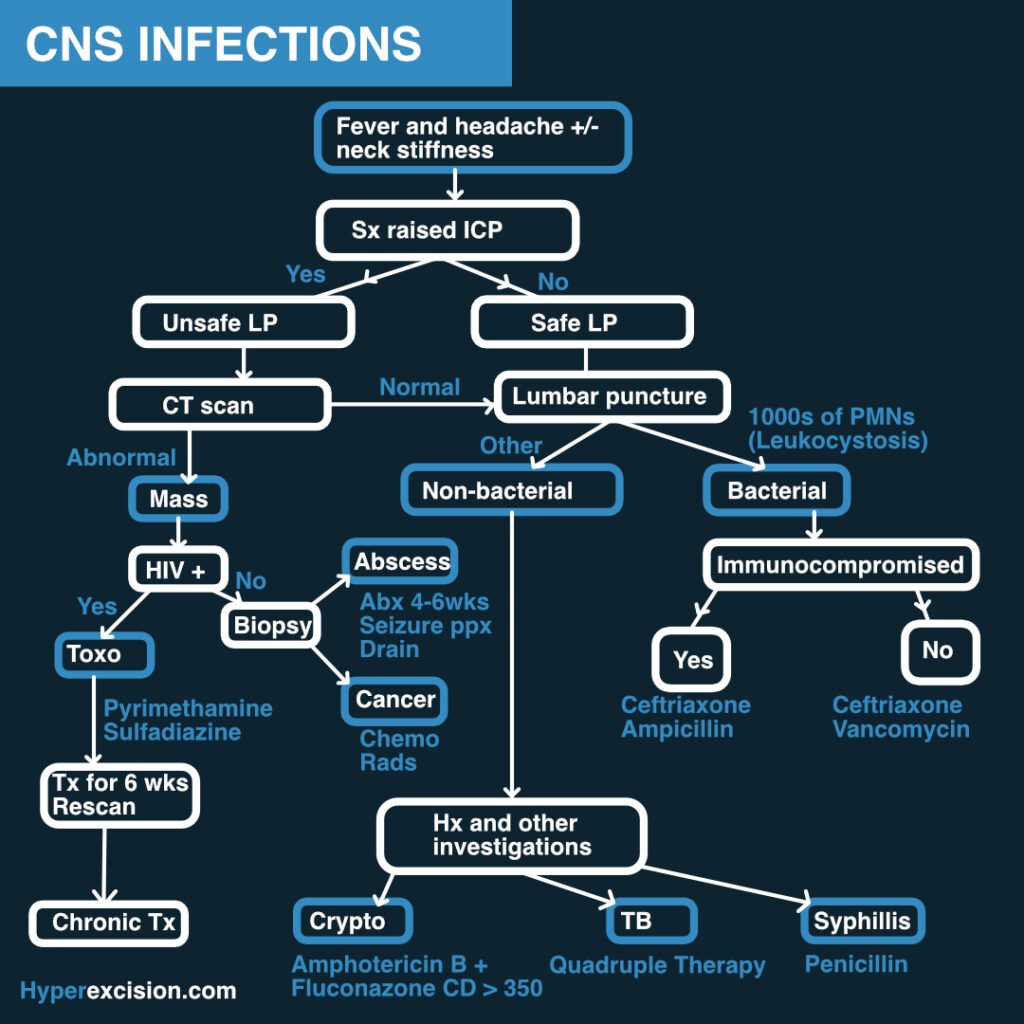
Overview
CNS infections carry a high mortality if untreated or improperly treated. It is important to recognize and treat differently neonates, young people, adults, old people, and immunocompromised since different organisms affect these different populations.
Infections of the CNS include:
| Infection | Description |
|---|---|
| Meningitis | Infection of the meninges |
| Encephalitis | Generalized infection of the brain parenchyma |
| Brain abscess | Focal infection and suppuration of the brain parenchyma |
- Symptom triad of CNS infections
- Fever
- Headache
- Altered mental status
Videos
Reference Intervals
›
Biochemistry
| ACTH | P: <80 ng/L |
| ALT | P: 5–35 U/L |
| Albumin | P: 35–50 g/L |
| Aldosterone | P: 100–500 pmol/L |
| Alk. phosphatase | P: 30–130 U/L |
| α-Amylase | P: 0–180 IU/dL |
| α-Fetoprotein | S: <10 kU/L |
| Angiotensin II | P: 5–35 pmol/L |
| ADH | P: 0.9–4.6 pmol/L |
| AST | P: 5–35 U/L |
| Bicarbonate | P: 24–30 mmol/L |
| Bilirubin | P: 3–17 μmol/L |
| BNP | P: <50 ng/L |
| CRP | P: <10 mg/L |
| Calcitonin | P: <0.1 mcg/L |
| Calcium (ionized) | P: 1.0–1.25 mmol/L |
| Calcium (total) | P: 2.12–2.60 mmol/L |
| Chloride | P: 95–105 mmol/L |
| Cholesterol | P: <5.0 mmol/L |
| VLDL | P: 0.128–0.645 mmol/L |
| LDL | P: <2.0 mmol/L |
| HDL | P: 0.9–1.93 mmol/L |
| Cortisol AM | P: 450–700 nmol/L |
| Cortisol Midnight | P: 80–280 nmol/L |
| CK ♂ | P: 25–195 U/L |
| CK ♀ | P: 25–170 U/L |
| Creatinine | P: 70–100 μmol/L |
| Ferritin | P: 12–200 mcg/L |
| Folate | S: 2.1 mcg/L |
| FSH | P: 2–8 U/L ♂; >25 menopause |
| GGT ♂ | P: 11–51 U/L |
| GGT ♀ | P: 7–33 U/L |
| Glucose (fasting) | P: 3.5–5.5 mmol/L |
| Growth hormone | P: <20 mu/L |
| HbA1C (DCCT) | B: 4–6% |
| HbA1C (IFCC) | B: 20–42 mmol/mol |
| Iron ♂ | S: 14–31 μmol/L |
| Iron ♀ | S: 11–30 μmol/L |
| Lactate (venous) | P: 0.6–2.4 mmol/L |
| Lactate (arterial) | P: 0.6–1.8 mmol/L |
| LDH | P: 70–250 U/L |
| LH | P: 3–16 U/L |
| Magnesium | P: 0.75–1.05 mmol/L |
| Osmolality | P: 278–305 mosmol/kg |
| PTH | P: 0.8–8.5 pmol/L |
| Potassium | P: 3.5–5.3 mmol/L |
| Prolactin ♂ | P: <450 U/L |
| Prolactin ♀ | P: <600 U/L |
| PSA | P: 0–4 mcg/mL |
| Protein (total) | P: 60–80 g/L |
| Red cell folate | B: 0.36–1.44 μmol/L |
| Renin (erect) | P: 2.8–4.5 pmol/mL/h |
| Renin (recumbent) | P: 1.1–2.7 pmol/mL/h |
| Sodium | P: 135–145 mmol/L |
| TBG | P: 7–17 mg/L |
| TSH | P: 0.5–4.2 mU/L |
| T4 | P: 70–140 nmol/L |
| Free T4 | P: 9–22 pmol/L |
| TIBC | S: 54–75 μmol/L |
| Triglycerides | P: 0.50–2.3 mmol/L |
| T3 | P: 1.2–3.0 nmol/L |
| Troponin T | P: <0.1 mcg/L |
| Urate ♂ | P: 210–480 μmol/L |
| Urate ♀ | P: 150–390 μmol/L |
| Urea | P: 2.5–6.7 mmol/L |
| Vitamin B12 | S: 0.13–0.68 nmol/L |
| Vitamin D | S: 50 nmol/L |
Arterial Blood Gases
| pH | 7.35–7.45 |
| PaCO₂ | 4.7–6.0 kPa |
| PaO₂ | >10.6 kPa |
| Base excess | ±2 mmol/L |
Urine
| Cortisol (free) | <280 nmol/24h |
| Hydroxyindole acetic acid | 16–73 μmol/24h |
| Hydroxymethylmandelic acid | 16–48 μmol/24h |
| Metanephrines | 0.03–0.69 μmol/mmol cr. |
| Osmolality | 350–1000 mosmol/kg |
| 17-Oxogenic steroids ♂ | 28–30 μmol/24h |
| 17-Oxogenic steroids ♀ | 21–66 μmol/24h |
| 17-Oxosteroids ♂ | 17–76 μmol/24h |
| 17-Oxosteroids ♀ | 14–59 μmol/24h |
| Phosphate (inorganic) | 15–50 mmol/24h |
| Potassium | 14–120 mmol/24h |
| Protein | <150 mg/24h |
| Protein/creatinine ratio | <3 mg/mmol |
| Sodium | 100–250 mmol/24h |
Haematology
| WCC | 4.0–11.0 ×10⁹/L |
| RBC ♂ | 4.5–6.5 ×10¹²/L |
| RBC ♀ | 3.9–5.6 ×10¹²/L |
| Hb ♂ | 130–180 g/L |
| Hb ♀ | 115–160 g/L |
| PCV ♂ | 0.4–0.54 L/L |
| PCV ♀ | 0.37–0.47 L/L |
| MCV | 76–96 fL |
| MCH | 27–32 pg |
| MCHC | 300–360 g/L |
| RDW | 11.6–14.6% |
| Neutrophils | 2.0–7.5 ×10⁹/L (40–75%) |
| Lymphocytes | 1.0–4.5 ×10⁹/L (20–45%) |
| Eosinophils | 0.04–0.44 ×10⁹/L (1–6%) |
| Basophils | 0–0.10 ×10⁹/L (0–1%) |
| Monocytes | 0.2–0.8 ×10⁹/L (2–10%) |
| Platelets | 150–400 ×10⁹/L |
| Reticulocytes | 0.8–2.0% / 25–100 ×10⁹/L |
| Prothrombin time | 10–14 s |
| APTT | 35–45 s |
Paediatric
| Pulse Rate (bpm) | |
|---|---|
| Neonate | 140–160 |
| Infant <1yr | 120–140 |
| 1–5 years | 110–130 |
| 5–12 years | 80–120 |
| >12 years | 70–100 |
| Respiratory Rate (tachypnoea) | |
| 0–2 months | ≥60/min |
| 2–12 months | ≥50/min |
| 1–5 years | ≥40/min |
| >5 years | ≥30/min |
| Blood Pressure (mmHg) | |
| Term | 65/45 |
| 1 year | 75/50 |
| 4 years | 85/60 |
| 8 years | 95/65 |
| 10 years | 100/70 |
| Weight Formulas | |
| 3–12 months | (a + 9)/2 kg |
| 1–6 years | 2a + 8 kg |
| >6 years | (7a − 5)/2 kg |
| Haemoglobin (g/dL) | |
| Term newborn | 13–20 |
| 1 month | 11–18 |
| 2 months | 10–15 |
| 1–2 years | 10–13 |
| >2 years | 11–14 |
| MUAC (6 months–5 years) | |
| Obese | >17.5 cm |
| Normal | 13.5–17.4 cm |
| At risk | 12.5–13.4 cm |
| Moderate malnutrition | 11.5–12.4 cm |
| Severe malnutrition | <11.5 cm |
| Developmental Milestones | |
| Social smile | 1.5 months |
| Head control | 4 months |
| Sits unsupported | 7 months |
| Crawls | 10 months |
| Stands unsupported | 10–12 months |
| Walks | 12–13 months |
| Talks | 18 months |
| CSF WBC (/mm³) | |
| Term newborn | 0–25 |
| >2 weeks | 0–5 |
Calculator
›