Overview
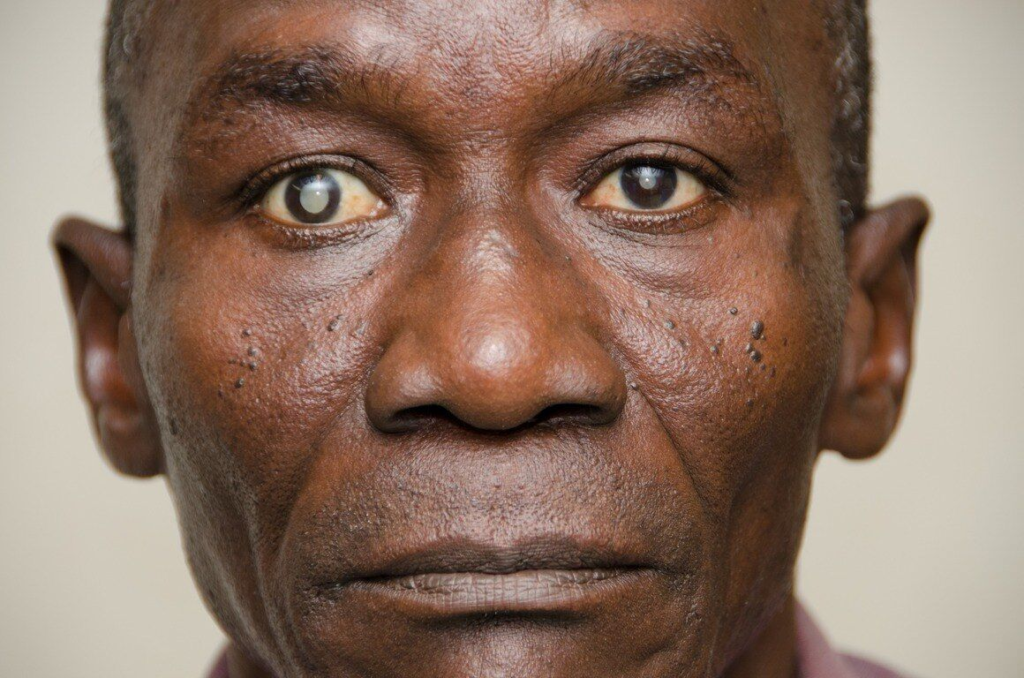
A cataract is an opacity of the crystalline lens. It causes haziness and cloudiness of vision. It is a painless process. It is treated by surgery.
- Common risk factors

Leukocoria
Leukocoria can be a presenting sign of cataracts. It appears as a “white pupil” on gross examination or via examination with an ophthalmoscope (with a lack of red reflex). Leukocoria in infants and children is alarming and is a medical emergency since it may indicate retinoblastoma.
- Differentials for leukocoria
- Retinoblastoma
- Congenital cataract
- Retinal malformation
- Retinopathy of prematurity
- Retinal detachment
- Intraocular infeciton
Congenital Cataract
Congenital cataracts are a major cause of vision loss in children worldwide and are the most common cause of leukocoria in children. The morphology of cataracts can provide clues towards the possible cause.
1/3 of congenital cataracts are hereditary. Another 1/3 is due to infection or congenital syndrome (Down syndrome, Alport syndrome). The remaining 1/3 is idiopathic.
- Causes of congenital cataracts
- Infectious (TORCH)
- Toxoplasmosis
- Other: Syphilis, Parvovirus B19
- Rubella: classically develop cataracts
- CMV
- HSV, HIV
- Genetic/metabolic errors (tend to have bilateral cataracts)
- Down syndrome
- Galactosemia (NBS)
- Lowe’s syndrome (urine calcium, phosphorus, amino acids)
- Alport’s syndrome (hearing deficit, renal impairment, X-linked)
- Fabry’s disease (skin manifestations, renal impairment, X-linked)
- Coat’s disease (unilateral, presents older, gradual vision loss)
- Infectious (TORCH)
- Pathophysiology of cataracts in galactosemia
- Aldose reductase is an enzyme involved in the polyol pathway that is involved in the breakdown of:
- Glucose to sorbitol
- Galactose to galactitol
- This enzyme normally has low levels of activity in the lens
- In galactosemia, the high galactose levels activate aldose reductase in the lens which increases the levels of galactitol produced
- Galactitol accumulates in the lens and draws in fluid leading to increased lens osmolarity which results in cataract formation
- Aldose reductase is an enzyme involved in the polyol pathway that is involved in the breakdown of:
- Signs and symptoms
- Leukocoria
- Absent red reflex (unilateral or bilateral)
- Nystagmus
- The child may be unaware of visual surroundings (especially if bilateral)
- Investigations
- Ophthalmologic
- Slit lamp examination
- Dilated fundoscopic examination
- Laboratory
- TORCH titers (Toxoplasmosis, CMV, VDRL)
- Urine for amino acids, phosphates, calcium
- Other routine labs (CBC, UECs)
- Ophthalmologic
- Treatment
- Surgical removal (no later than 3 months of age)
- Followup with ophthalmology and optometry
- Genetic counseling if appropriate
- Complications of congenital cataracts
- Deprivation amblyopia
- Strabismus
- Blindness
Senile Cataract
Senile cataracts occur with age and are the leading cause of blindness worldwide. Cataracts are reversible. However, the lens can begin to irreversibly thicken as the cataract matures.
Mature cataract: The patient cannot read better than 20/200 (6/60)
Immature cataract: The patient cannot see better than 20/20 (6/6)
Incipient cataract: The patient can see 20/20 (6/6)
Most patients over 60 years of age have some degree of cataract.

- Risk factors
- Advanced age
- Cigarette smoking
- Diabetes mellitus
- Alcohol
- Hyperlipidemia
- Hypertension
- Hyperglycemia
- Excessive UV exposure
- Pathophysiology of cataracts in diabetes
- Aldose reductase is an enzyme involved in the polyol pathway that is involved in the breakdown of:
- Glucose to sorbitol
- Galactose to galactitol
- This enzyme normally has low levels of activity in the lens
- In diabetes, the high glucose levels activate aldose reductase in the lens which increases the levels of sorbitol produced
- Sorbitol accumulates in the lens and draws in fluid leading to increased lens osmolarity which results in cataract formation
- Aldose reductase is an enzyme involved in the polyol pathway that is involved in the breakdown of:
- Signs and symptoms
- Visual impairment (chief complaint)
- Leukocoria
- Glare/halos
- Myopic shift (increase in the convergence power of the lens. Ask the patient whether they are using their reading glasses as much as they did before)
- Monocular diplopia (a double vision that does not go away when you cover one eye)
- Physical examination Examined in a brightly lit room
- Ophthalmoscopic exam
- Slit-lamp examination (for a formal and more precise diagnosis)
- Investigations Assess for possible concurrent illnesses that can contribute to cataract formation
- Random Blood Glucose, Fasting blood glucose, HbA1C
- Lipid panel
- Treatment
- Surgical removal by an ophthalmologist
- Prognosis
- 95% of adults have increased visual acuity following surgery
Other causes of Cataracts in adults
- Ocular trauma
- Radiation
- Adverse effects of corticosteroids, antipsychotics (Quetiapine)
- Skin diseases: Atopic dermatitis, Eczema