Pulmonary edema where the heart is to blame. Increases in pulmonary pressure (PCWP) are secondary to ineffective filling/pumping of the heart. This is the most common presentation of Congestive Heart Failure (CHF).
The patient is being hospitalized and is a few days post MI, develops sudden dyspnea, pink frothy sputum, and new systolic murmur
Papillary muscle rupture
The patient is very tachycardic, presents with anxiety, chest pain, and SOB, and has an EKG that shows wide QRS complexes with no discernable P or T waves
Ventricular Tachycardia
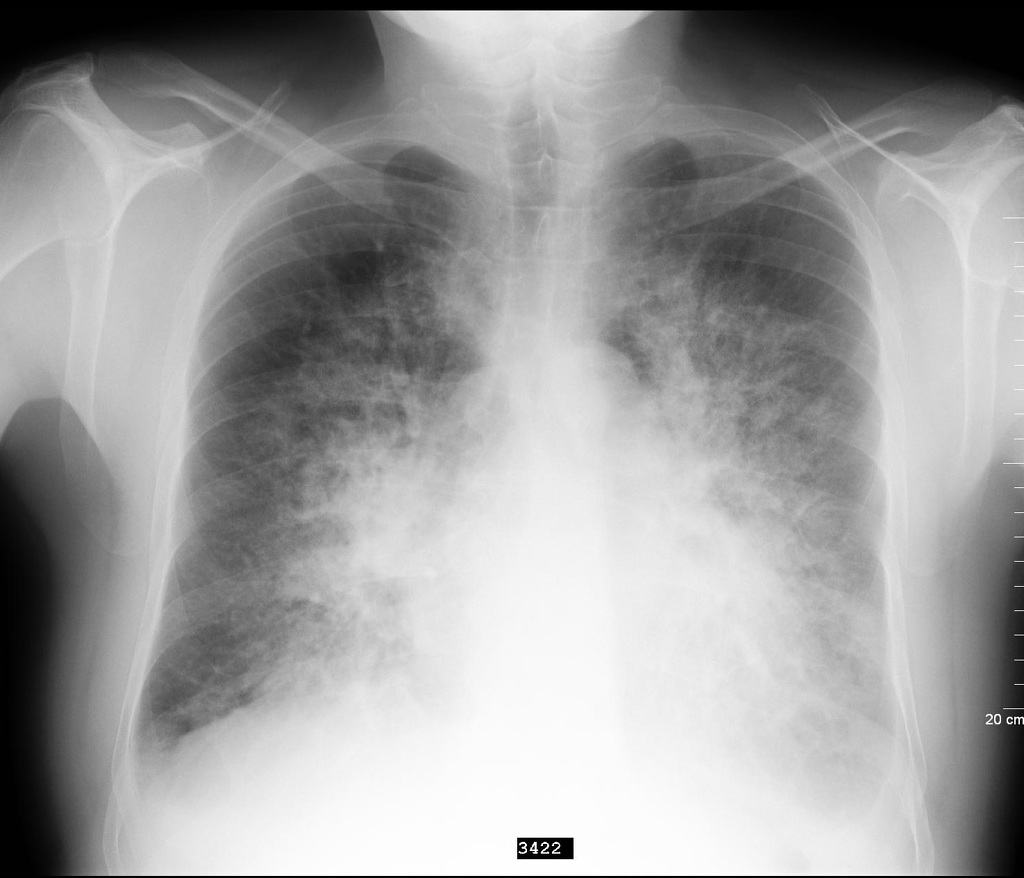
Chest X-ray in pulmonary Edema
Chest X-ray will clue you in on whether the edema is cardiogenic or non-cardiogenic. History, presentation, labs, and often echo and EKG are needed for definitive diagnosis
Chest X-ray findings in acute pulmonary oedema
Alveolar infiltrates: a must with every pulmonary edema (wheezing, hypoxia, etc.) – “Bat’s wings”
Kerley B lines: fluid infiltration onto pulmonary interstitium (needs a keen eye)
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.