Tissue: presence of granulation or hypergranulation tissue, devitalized or necrotic tissue, and surrounding tissue
Inflammation or infection: areas within or surrounding the wound site that may indicate the presence of infection or inflammation
Moisture: moisture balance and whether the wound is dry or macerated
Edge of the wound: assess for re-epithelialization vs non-advancing ages vs epibole. Also assess blood supply to the edges of the wound.
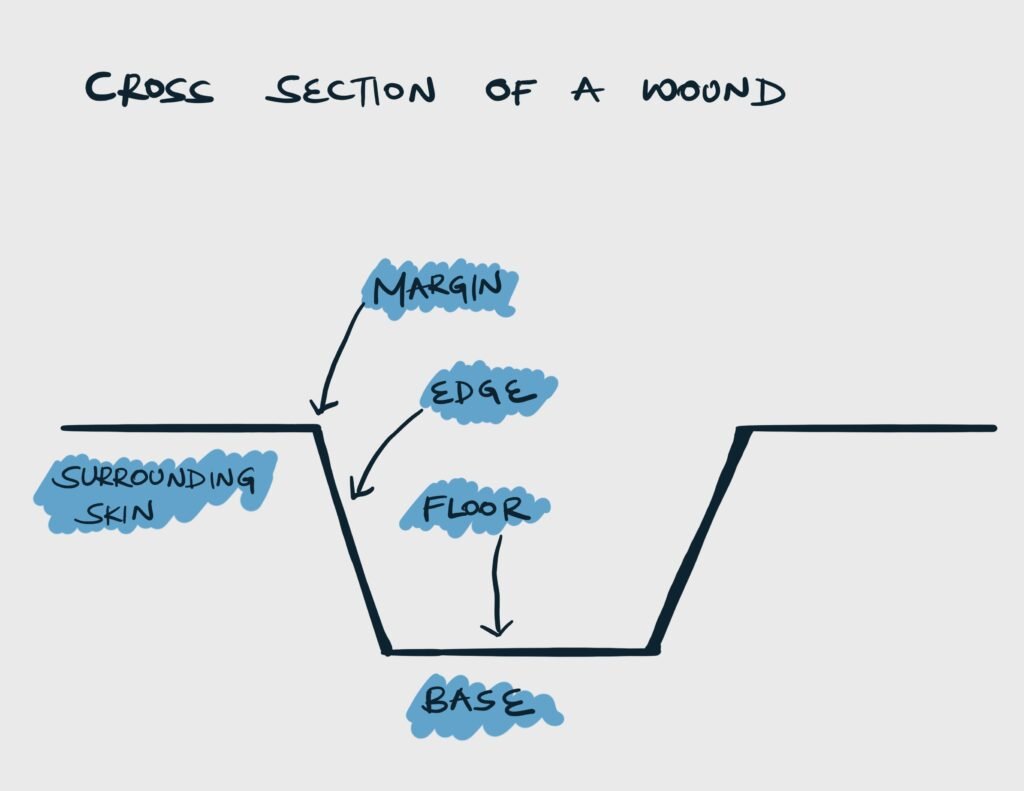
Parts of a wound
Part
Definition
Description
Marging
A line that represents the junction between instact skin and the ulcer
Rounded or oval. Regular or Irregular. Well-defined or ill-defined.
Edge
The block of tissue that connects the margin and the floor of the ulcer
Sloping, undermined, punched out, raised and beaded, or everted
Floor
Visible part overlying the base
Contanins discharge, granulation tissue (red/pink) or slough (yellow)
Base
Tissue on which the ulcer rests on
Bone, tendons, or muscle
Crosss section of a wound
Size
Wound size should be measured and documented on first presentation and regularly after that. Dimensions include length, width and depth of tissue planes. Wounds can be measured using a tape, ruler, scalpel handle or gloved finger.
Margin
Margin
Inference
Ill-defined irregular margins
Growing or spreading ulcer
Well-defined regular white margin
Non-healing ulcer
Well-defined regular margin with white, blue, and red zones
Epibole: a rolled or curled-under wound edge where the epithelial layer fails to advance. The upper epidermal edge moves over the lower edge causing epithelialization down the wound edge rather than across the base. They must be resected or debrided in order for epithelialization to continue.
Floor
Floor content
Inference
Pink with tiny red granules or nodules (capillary “buds”)
Healthy granulation
Pale flat granulation, “heaped up” appearance
Unhealthy granulation, exuberant granulation
Scanty serous discharge
Can be seen in healthy granulation
Yellow, white, or grey slough
Infection has not been controlled and granulation is yet to begin
Serosanguinous purulent discharge
Infected ulcer
Dry, hard, or leathery, and black
Eschar
Surrounding skin
Inspect the surrounding skin for cellulitis, maceration, and other peri-wound skin abnormalities e.g. scars, deformities, rashes, and varicosities.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.