Overview
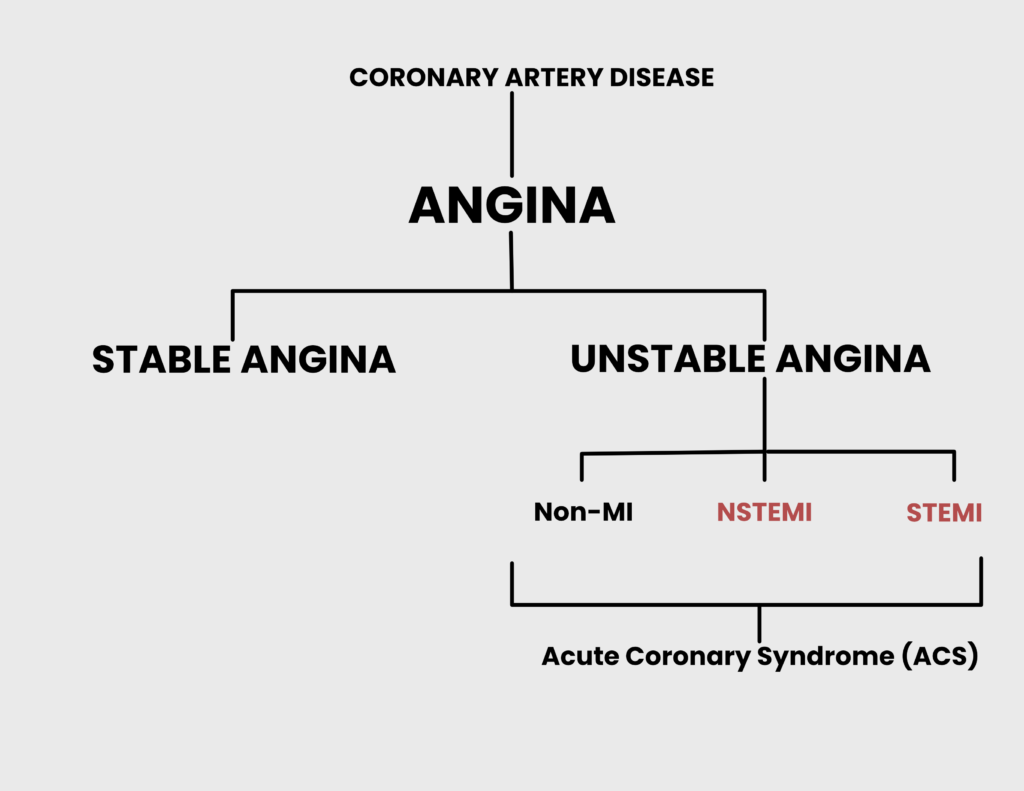
Angina refers to chest pain on exertion. The chest pain is always sub-sternal, and is described as crushing/heavy, lasts minutes to hours, and may radiate to the upper arm or shoulder. 99% of cases are due to coronary artery disease. However, the transient period of ischemia is insufficient to cause necrosis. Episodes last less than 3 minutes and may be relieved with rest. Episodes >30 minutes are suspicious for unstable angina. The basic pathophysiology is that oxygen demand in the cardiomyocytes outweighs supply.
It is common in middle-aged and elderly men. Women are usually affected post-menopause. 10-20% of individuals with angina develop myocardial infarction or unstable angina within 1 year of diagnosis of stable angina
| Term | Definition |
|---|---|
| Stable angina | Chest pain on exertion that is relieved with rest |
| Unstable angina | Chest pain on exertion that is NOT relieved with rest or Chest pain that is new or worse than previous episodes |
| Prinzmetal’s angina | Cyclical chest pain that may occur during rest. Due to vasospasm |
| Decubitus angina | Chest pain precipitated by lying flat |
Bottomline treatment of ACS
| Treatment | When to use it | Treatment goal |
|---|---|---|
| Statin | Any ACS | LDL < 70 and HDL > 40 |
| Beta Blocker | Any ACS | SBP < 140 and DBP < 90 |
| ACEi/ARB | Any ACS | SBP < 140 and DBP < 90 |
| Aspirin | Any ACS | No goal |
| Clopidogrel | Aspirin allergy or drug-elluting stent | |
| tPA | ST elevation or positive stress test when PCI or transport is unavailable | |
| Heparin | ST elevation or positive stress test when tPA is contraindicated | |
| Angioplasty (PCI) | ST elevation or positive stress test, 1 or 2 vessel disease | |
| CABG | ST elevation or ositive stress test, Left-mainstem or 3 vessel disease |
Pathogenesis
- Risk factors for angina
- Modifiable
- Cholesterol level (Target LDL < 100; <70 if diabetic)
- Smoking
- Hypertension
- Diabetes Mellitus
- Obesity
- Sedentary lifestyle
- Non-modifiable
- Age >60 years
- Male gender
- Family History of Angina
- Modifiable
- Causes of angina
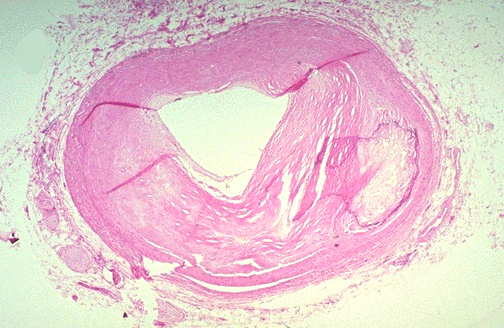
- Atherosclerosis of the coronary arteries (MCC, critical stenosis occurs at 70% occlusion)
- Anaemia
- Aortic steonosis
- Tachyarrhythmia
- Atrioventricular stenosis
- Hypertension with Left Ventricular Hypertrophy
- Hypertrophic Cardiomyopathy
- Cocaine-induced coronary artery vasospasms
- Pathophysiology
- Fixed atheromas cause vaso-occlusion → reduced coronary artery blood flow → increased oxygen demand during exertion → Subendocardial ischemia
- Hypertension → Concentric hypertrophy of the left ventricle → increased oxygen demand and hypoxia
- Thrombosis after rupture of atheromatous plaque → increased release of Thromboxane A2 from platelets and endothelin from endothelial cells → Vasoconstriction → ischemia
Clinical Features
- Signs and symptoms
- Chest pain
- Substernal
- Lasting 30 seconds to about 30 minutes
- Induced by exercise/sexual intercourse/climbing stairs/eating a heavy meal/emotional stress/cold temperature
- Relieved by resting or Nitroglycerin
- Associated with breathlessness, sweating, nausea, or numbness and pain radiating to the upper arm or shoulder
- Chest pain
Investigations
- Investigations
- Electrocardiogram
- ST-segment depression = subendocardial ischemia
- Flat or inverted T-waves
- Lipid panel
- If LDL >100 or 70 in diabetic start the patient on a Statin.
- Complete blood count: usually within normal limits
- Fasting blood glucose and HbA1C for Diabetes or pre-diabetes
- Consider Chest-Xray and Echocardiogram
- Angiography
- Vasospasm of coronary arteries = Prinzmetal angina
- Ergonovine challenge
- Exacerbates pain in Prinzmetal angina
- Functional imaging (exercise echo/myocardial perfusion scintigraphy/cardiac MRI)
- Electrocardiogram
Exercise Stress Test
A stress test is used to determine the severity of the disease in patients who have been diagnosed with angina. The results are used to determine whether the patient will need invasive treatment (after angiography). A chemical stress test is preferred over an exercise stress test in patients whose exercise stress test is not possible or have a pre-existing arrhythmia.
| Stress test | Description |
|---|---|
| Exercise stress test | The patient is monitored on an EKG until they reach 80% of maximum heart rate (220 – age in years) |
| Chemical stress test | Dobutamine echo stress test and Dipyridamole-Thallium scintigraphy |
- Positive exercise stress test
- Ischemia = ST depression ≥ 2mm
- Hypotension = drop in systolic bP ≥ 10 mmHg
- Positive Dobutamine echo stress test
- Decreased cardiac wall movement
- Positive Thallium scintigraphy
- Decreased uptake of Thallium (thallium is identical to potassium and is taken up by myocytes)
Angiography
All patients with a positive stress test require an angiogram to determine the extent and severity of atherosclerosis. Patients subsequently require angioplasty with stenting (Percutaneous intervention – PCI) or Coronary artery bypass graft (CABG)
- Indications for CABG in stable angina
- 3 vessel disease
- Left main artery disease
Treatment of Stable Angina
The goal of treatment of angina is to reduce the risk of cardiovascular events (myocardial infarction, stroke, and death) and to improve quality of life by reducing symptoms of angina
Take into consideration the patient’s modifiable risk factors when prescribing treatment IE. hyperlipidemia, hypertension, smoking, weight, and lifestyle.
- Indications for statin
- Coronary artery disease
- Peripheral artery disease
- Aortic disease
- Carotid disease
- Cerebrovascular disease
- Diabetes + LDL > 100mg/dL.
- Atherosclerotic Cardiovascular Disease 10-year risk > 7.5%
- Treatment
- Address exacerbating factors e.g. anemia, tachyarrhythmia
- Secondary prevention
- Daily Low-dose Aspirin or Clopidogrel (has a mortality benefit 😃)
- Statin (Artovastatin) if LDL > 100mg/dL.
- Target < 70mg/dL if diabetic
- Target < 100mg/dL if non-diabetic
- ACEi (Captopril, Lisinopril) if Diabetic
- Lifestyle modification: Diet and exercise, weight loss, smoking cessation
- Symptom relief
- Nitroglycerin PRN
- Side effects → headache, postural hypotension
- Repeat dose of pain does not go away in 5 minutes
- Call an ambulance if the pain does not go away within 5 minutes after the second dose
- Nitroglycerin PRN
- Anti-anginal medicationsDo not combine Beta-blockers with non-dihydropyridine CCBs!
- Beta-blocker (Metoprolol, Atenolol, Bisoprolol): first-line
- Calcium channel blocker (Amlodipine, Dilitiazem): a first-line alternative to beta-blockers
- Long-acting nitrate (Isosorbide mononitrate)
- Side-effects → headache and postural hypotension
- Ivabradine (reduces HR with minimal effect on BP)
- patient must be in sinus rhythm before starting
- Ranolazine (inhibits late Na+ current)
- Use with caution if there is heart failure, elderly, weight <60kg or elderly
- Nicorandil (activates K+ channels)
- Contraindicated in acute pulmonary edema, severe hypotension, hypovolemia, LV failure
- Revascularization
- Percutaneous intervention (PCI)
- Coronary artery bypass graft (CABG)