Table Of Contents
Haemophilus
- Briefly describe Haemophilus
- Haemophilus is derived from the roots “Haemo” (Blood) and “hilos” (loving). Haemophilus is thus a “blood loving” gram negative plemorphic coccobacilli that is non-motile.
- Hemophilus can be either aerobic or facultatively anerobic.
- It is part of the normal flora of the human mouth and Respiratory tract.
- Hemophilus is oxidase positive and growth in culture requires X-factor (Unknown factor, Hematin) and V-factor (Vitamin factor, NAD).
- It shows no growth in MAC due to lack of X factor and V-factor.
- Common species include:
- Hemophilus influenzae (Meningitis, epiglottitis, pneumonia)
- Hemophilus parainfluenzae,
- Hemophilus ducreyi (Soft chancre/chancroid)
- *Hemophilus influenzae biogroup aegypticus ****(*Biotype II, acute purulent conjunctivitis)
- Briefly describe Hemophilus influenzae
- Hemophilus infuenza was first described in 1892 by Richard pfeiffer during the influenza pandemic.
- It is a non-motile, gram negative rod that is aneorbic/ facultative anerobic, catalas positve and oxidase positive.
- It has encapsulated (typable -A,B,C,D,E,F; B being most pathogenic) and unencapsulate (non-typeable) strains.
- It is also subdivided into 8 biotypes (according to indole production, urease activity and ornithine decarboxylase activity)
- Hemophilus influenzae is sensitive to cold temperatures (non-viable at 0-4*C).
- Outline the virulence factors associated with Haemophilus influenzae
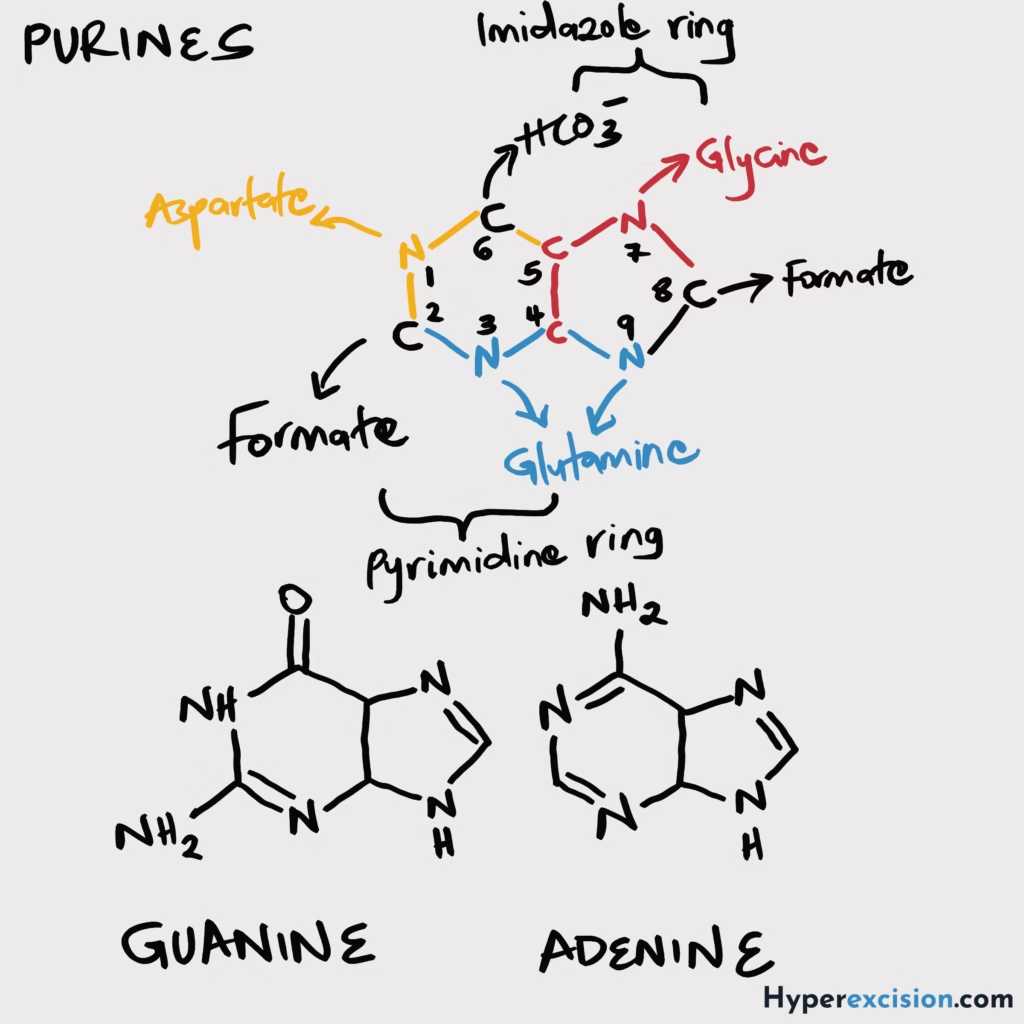
- Capsule: Antiphagocytic, resists complement-mediated lysis, contains Polyribitol phosphate (PRP) **** ***Non-encapsulated strains of H.influenzae and H.parainfluenzae colonize the URT (opportunistic infections) of virtually all people (50-75%) in the first few months of life. They can spread locally to cause otitis media, sinusitis, chronic bronchitis (adults), pneumonia and conjunctivitis. Disseminated disease is uncommon ***Encapsulated HiB is an uncommon URT flora and is present in only very small numbers (2-4%). It is a common cause of disease in unvaccinated children.
- Endotoxin: Inflammation
- IgA Protease: Mucosal colonization
- Neuraminidase: Mucosal colonization
- What groups of individuals are at risk of infections with Haemophilus influenzae
- Inadequate levels of protective Abs
- Complement deficiency
- Status post splenectomy
- Immunocompromised patients
- Outline the clinical features of Haemophilus influenzae
- Pyogenic meningitis: Children 2 months – 5y
- Epiglottitis: Unimmunized children, less common than miningitis, pharyngitis, fever and DIB that progresses to cellulitis and sweling of supraglottic tissue with obstructive laryngitis
- Pneumonia: bronchopneumonia in the elderly with underlying chronic pulmonary disase, typically caused by non-typeable strains
- Suppurative arthritis
- Otitis media
- Cellulitis
- Outline the laboratory features of Haemophilus influenzae
- Specimen: CSF, Blood, Pus swab, Sputum
- Primary isolation: Fildes agar (added peptic digest of blood to nutrient agar, gives copious growth)
- Culture: CBA with factor X and V, temp of 37*C, 5-10% CO2 enriched incubator, 18-24 hours, colonies are pinpoint (1-3mm), convx, smooth and mucoid (encapsulated)
- Gram stain: Gram negative coccobacily with school of fish appearance (small clusters of parallel chains of 2 or more organisms)
- Biochemical tests
- Catalase: Positive
- Oxidase: Positive
- Satteitism test: grows around colonies of S. aureus on unheated blood Agar. HiB colonies are smaller than on CBA since V factor inhibitors present in blood are not inactivated.
- Demonstration of growth factor requirements: Grows areound strips with factors X and V together
- Latex particle agglutination: PRP capsular antigen in CSF and urine, rapid and sensitive, limited to HiB
- Biotyping
- Electrophoretic characterization of membrane protein antigens
- PCR
- Briefly describe the prevention and control of Haemophilus influenzae
- Know the antibiotics.
- Also remember the capsular polysaccharide conjugate vaccine that part of the DPT-HepB-HiB pentavalent vaccine under KEPI
- Briefly describe Haemophilus ducreyi
- Haemophilus ducreyi is a fastidious gram negative coccobacilus that is found in humans only during disease (not normal flora).
- It is more fastidious than HiB (CBA is supplemented with Isovitalex for culture)
- It causes soft sore (chancroid, softer than syphilitic shancher).
- Lacks ferrochetalase and cannot synthesize heme
- List the virulence factors associated with Haemophilus ducreyi
- Peptidoglycan associated lipoprotein
- Pili
- Cytotlethal distending toxin (HdCDT): induced DNA damage and cell cycle arrest → apoptosis
- Pathogenesis
- Infects skin breaks → Stimulates macrophages lymphocytes granulocytes and inflammation → HdCDT causes apoptosis → Pyogenc inflammation causes regional lymphadenitis
- Briefly describe the clinical features of Chancroid
- Mostly diagnosed in men. Women have asymptomatic disease.
- Forms a tender papulae with an erythemaotus base on the genitalia and perianal area.
- Within 2 days the ulcerate, become painful and show inguinal lymphadenopathy.
- 40% suppurate (painfule genital adenitis, buboes)
- Outline the laboratory features of Haemophilus ducreyi
- Specimen: Ulcerated chancorid exudate (from base and margins, on swab, place in Amie’s transport mediu)
- Culture: CBA with isovitalex and vancomycin, Microaerophilic, 33-35*C, jumid atmosphere, 5% CO2 for 4 8hours, small, grey-tan yellow or brown collonies, highly self adherent can be nudged intact over agar surdace
- Gram stain: Bacilli in clusters or small chains (School of fish)
- PCR
- Briefly describe Hemophilus parainfluenzae
- He is a low virulence rod that causes sporadic endocarditis and pyogenic arthritis
- Briefly describe Haemophilus aegypticus
- AKA Koch-weeks bacillus
- Haemophilus aegypticus causes acute purulent conjunctivitis and is associated with epidemics during the warm months of the year.
- It also requires X and V factors.
- Causes brazilian purpuric fever (conjunctivitis that leads to fulminant septicemia – has a high mortality)
- List 2 characteristics associated with Hemophilus hemolyticus
- Shows B-hemolysis on BA and is an URT commensal
- List 5 diseases caused by Hemophilus aphrophilus
- Septicemia
- Endocarditis
- Meningitis
- Brain abscesses
- Pneumonia
Differentiate Hemophilus species according to factor X and V requirements
| Factor X | Factor V | |
|---|---|---|
| H. influenzae | + | + |
| H. parainfluenzae | – | + |
| H. ducreyi | + | – |
| H. aegyptius | + | + |
Bordetella
- Briefly describe Bordetella
- Bordetella is a small GN coccobacillus occurring singly or in pairs.
- He is an obligate aerobe that **does not ferment CHOs (**AAs are energy source) and is catalase positive.
- Species of importance include:
- Bordetella pertusis (Whooping cough)
- Bordetella parapertussis (Milder pertussis)
- Bordetella bronchiseptica (Respiratory Tract of dogs, swines and humans).
- Briefly describe Bordetella pertussis
- Bordetella pertussis is encapsulated (especially when freshly isolated), piliated, non-motile, non-spore forming, and sensitive to drying.
- It causes pertussis in humans and has no animal of environmental reservoir
- Bordetella pertussis is encapsulated (especially when freshly isolated), piliated, non-motile, non-spore forming, and sensitive to drying.
- How is Bordetella pertussis transmitted
- Inhalation of infectious aerosols
- Briefly describe the epidemiology of Bordetella pertussis
- Incidence, morbidity and mortality have reduced after the vaccine was introduced.
- Pertussis is a human disease with no known animal or environmental reservoir.
- It has a worldwide distribution (roughly 16 million infections and 200K deaths each year primarily in unvaccinated children).
- Children <1 year are at greast risk for infection and mortality.
- Diseases in vaccinated population occur in older children and yound adults.
- List the virulence factors associated with Bordetella pertussis
- Petractin: adhesin
- Pili (fimbriae): adhesin
- Filamentous hemagglutinin: adhesin
- Pertusiss toxin: elevated cAMP → inc Respiratory secretions and mucus production → characteristic of paroxysmal stage of pertussis, promotes lymphocytosis
- Tracheal cytotoxin: damages cilia (disrupts clearance and contributes to pertusis cough) and stimulates IL-1 release (fever)
- Highly-lethal toxin (dermonecrotic toxin): Inflammation and local necrosis
- Briefly describe the pathogenesis of Whooping cough
- Colonization of lung epithelial cells
- Pili and hemagglutinins bind to sulfatides of cilia
- Binding to PMNs initiates phagocytosis protecting the bacteria from humoral Antibodies
- Tracheal cytotoxin paralyzes cilia leading to paroxysmal of coughs and impaired removal of excess mucus
- Pertussis toxins promotes lymphocytosis and mucus secretion (initiated cough spasms)
- Outline the clinical features of Whooping cough ***Classical presentation isn;t seen in patiens with partial immunity or adults
- Incubation (5-10 days, max 21)
- Catarrhal phase (1-2 weeks): Low grade fever, catarrhal symptoms (rhinitis, blocked nose, postnasal drip), throat irritation, facial pain, h’ache, anosmia, loss of tae, Most risky (high bacterial load)
- Paroxysmal phase (1-6 weeks): increase cough intensity and frequency, Whoop (long intake of air, rushing into empty lungs), fluid streams from eyes ose, mouth +/- voimiting and convulsions, as many as 40-50 paroxysms daily at height of illness
- Conavlescent phase (after 2-4 weeks, lasts weeks to months): Cough intensity decreased gradually,
- What are the complications of pertussis
- Encephalitis
- Bronchopneumonia
- Mental retardation
- Outline the laboratory features of Bordetella pertusis
- Specimen: Nasopharyngeal swabs, aspirates (from posterior nasopharynx, obtained using Dacron or Cotton swabs since he is sensitive to drying). cough droplets (culture plate coughed into)
- Gram smear: GN coccobacili
- Culture: Bordet-Gengou (selective and enriched) > Charcoal cephalexin BA, INcubate 35-37*C for 2-6 days in most aerobic conditions, Small rain drop like or mercury-like mucoid colonies
- Biochemical tests
- Urease: Negative
- Oxidase: Positive
- Nitrate: Negative
- PCR: highly sensitive (upto 4 weeks before bacterial DNA diminished)
- Serology: detects serovers (2-8 weeks post cough onset, useful upto 12 weeks)
- ELISA: Detects Abs against pertussis toxin, filamentous hemagglutinin, pertactin and fimbriae
- Outline the growth requirements of Bordetella
- Strict aerobe
- Media should be nutritionally enriched with blood
- Highly susceptibl to toxic substances and metabolies (in common lab media, cupplement these with charcoal, starch, blood or albumin to absrob them)
- Selective media for primary isolation: Modified Bordet-gengou
- Slow growth (2-4 days)
- What are the components of Modified Bordet-gengou agar
- Starch
- Glycerol
- Blood
- penicillin (inhibits growth of other organisms)
- Briefly describe Bordetella parapertussis
- Bordetella parapertussis is a non-motile, non-sporing, encapsulated rod that has similar morphology and antigenicity as Bordetella pertusis.
- It causes a milder form of whooping cough, grows relatively rapidly on BA, CBA (but not on MAC) and has larger colonies than pertusis
- Briefly describe Bordetella bronchiseptica
- Bordetella bronchiseptica is mainly an animal pathogen.
- It is a non-spore former, non-capsulated, motile rod found in the Respiratory Treact of domestic and wild animals.
- It is transmitted by infectious aerosols and is associated with pertussis like Respiratory Tract Infections in humans (pneumonia) and wound infections.
- Displays rapid growth on BA and MAC with small B-hemolytic colonies on MAC after 2-3 days at 35-37*C.
- Differentiate between the species of Bordetella through their identifying characteristics Pertussis Parapertussis Bronchiseptica Oxidase + – + Urease – + (slow) + Growth on NA – + + Growth on BA – + +
Legionella
- Briefly describe Legionella
- There was an outbreak of severe pneumonia among American Legion members attending a conventian in Philadelphia (1976). . After months of intensive investigations a previously unknown GNR was isolated and subsequent studies found and named this organisms Legionella pneumophila (the cause of multiple epidemics and sporadic infections). This organism was found to stain poorly with conventional dyes and did not grow on common lab media.
- Legionallea is a gram negative short bacillus/ coccobacillus, that is aerobic, motile and non-spore forming.
- Its natural habitat is water.
- *Legionella pneumophila *****accounts for 80-90% of legionella pneumonia cases.
- It has 16 serogroups (group 1 being the most pathogenic).
- 30 other species, including *Legionell micdadei, Legionella bozemanii *****cause the remaining 10% of pneumonia cases.
- Man does not normally carry legionella.
- 3 subspecies have been identified:
- Legionella pneumophilla ssp pneumophila,
- Legionella pneumophilla spp fraseri (described in human disease) ****
- Legionella pneumophila spp pascullei.
- The GN cell wall of legionella stains poorly (or not at all) with gram stain, but clinical specimen can be seen in tissues with silver impregnation methods (Dieterle silver impregnation stain).
- In biological material (sputum, lung or water deposits), legionella appears as short rods or coccobacilli
- In culture they become longer and sometimes filamentous.
- Legionella is an obligate aerobe.
- It is nutritionally fastidious (requires specific Amino Acids such as L-cysteine and ferric ions to enhance growth) and is a facultative intracellular organism (can survive in amoebae under adverse environmental conditions when they encyst).
- Legionella cannot grow on BA, does not ferment of oxidise CHO (energy is from AAs), and its major virulence factor is LPS endotoxin (has no exotoxin)
- Briefly describe the epidemiology of Legionella
- Legionella has a worldwide distribution, commonly occuring in natural bodies of water (lakes, streams, air conditioning cooling towers, condensers, showers, hot tubs),
- It can survive in moist envronment for long times at relatively high temp and at the presence of disinfectants (such as chlorine)
- It survives because it parasitizes amoeba and replicates in protected environment (similar to human macrophages).
- Legionella can also survive in biofilms that develop in the pipes of water systems.
- There are sporadic outbreaks throughout the year and most epidemics occur in the late summer or autumn when the organism proliferates in water reservoirs during the warm month.
- 90% of infections in the US are persons >40y (Due to decreased cellular immunity and compromised pulmonary function).
- A significant of reported cases are **nosocomial (**Asymptomatic are common, symptomatic infections affect the lungs)
- How is Legionella transmitted
- Inhalation of contaminated aerosols (spas, showers, air-conditioning, water storage tanks, respiratory therapy equipment)
- Favourable conditions invlude:
- temperatures outside normal (<20 C or >55 C)
- Flow obstruction
- Biofilm.
- No person-person transmissions
- Outbreaks can occur
- Briefly describe the pathogenesis of Pneumonia caused by Legionella
- Multiplicationn in free-living amoeba and alveolar macrophages/monocytes/epithelial cells
- Outer membrane porin protein binds to complement component C3b
- Complex binds fo CR3 complement receptor on mononuclear phagocytes
- Endocytosis and replication
- Inhibition of phagolysosome fusion
- Stimulation of an inflammatory response by infected macrophages (release of chemokines and cytokines)
- Produce proteolytic enzymes (phosphatase, lipase, nuclease) in intracellular vacules that kill host cell when the vacuole is lysed
- Immunity is Cell-mediated (humoral only plays a minor role)
- Production of IFN-y is crtitical for elimination of Legionella (esp after TH1 activates the parasitized macrophage)
- Outline the clinical features of Legionella
- Legionnaires disease: Legionnares disease is an atypical bronchopneumonia (rapidly progressive, scanty, non-purulent sputum). 15% mortality in healthy subjects. Higher nosocomial infection rates and 75% in immunocompromised. Characterized by confusion, hallucination and focal neurological signs, proteinuria and hematuria. **Hyponatremia (**Na ≤130mEq/L, secondatry to renal involvement) is an imortant indicator of legionella pneumonia. Predisposing factors include smoking, hospitalization, DM, immunosuppression, Renal CVS disease, Increase in age with a peak at 60-70y. ***different due to renal (proteinuria, hematuria, hyponatremia) and CNS involvement (confusion, hallucination and focal neurological signs)
- Pontiac fever: Mild influenza-like illness, low mortality and self-limiting. Derived from city in Michigan (Outbreak site in 1968)
- Rare Extrapulmonary: Nosocomial infections → Prosthetic valve endocarditis or Wound infection
- Outline the laboratory features of Legionella
- Specimen: Sputum, Bronchoalveolar lavage specimen, lung tissue, pleural fluid, wound swab, blood
- Microscopy: GN short rods or Coccobacilli
- Sputum gram stain: Many neutrophils, no bacteria (preferreed Fluorescent Ab Stain, Silver impregnation stain)
- Cultures
- Buffered Charcoal Yeast Extract (BCYE): Ground glass appearance of colonies (sensitivity depends on technical skill)
- Antiegns detection
- Legionella Urinary Ag test: positive days-weeks after treatment for Legionella pneumophila serogroup 1 (is a rapid test, same day results, does not allow for molecular comparisons to environmental isolates)
- Serology (Paired sera collecteed at acute onset to 2 weeks after symptoms and 3-6 weeks later, >4-fold rise or titre 1:256 is diagnositc, may take >8 days to develop after infection onset, cross reactivity with campylobacter, may persist for months/years post-infection)
- Serogroup identification
- Slide agglutination
- Direct Fluorescent antibody (DFA) test (techical difficuty, reagents aren’t easty to obtain)
- PCR (Rapid, assays vary, limited commercial availability, can use on tissue samples, for source identification, molecular and serological tests can be done on clinical and environmental samples)
- Why does Legionella require Buffered Charcoal Yeast Extract (BCYE) media for growth
- BCYE has Iron and Cysteine which is required by Legionella for growth
- Legionella is grown for 5-10 days, in 5-10% CO2
Compare and contrast Legionnaires disease and Pontiac fever
| Legionnaire’s Disease | Pontiac Fever | |
|---|---|---|
| Incubation | Longer (2-14 days) | Shorter (24-72 hours) |
| Clinical features | Pneumonia + cough, fever | Flu-like illness (fever, chills and malaise) without pneumoia |
| Pneumonia | Yes | No |
| Hospitalization | Common | Uncommon |
| Attack rate | < 5% | > 90% |
| Case-fatality rate | 5 – 30% | 0% |
| Isolation of organism | Possible | Cannot be isolated |